SMART NT Step Two:
Targeted scan to detect structural anomalies, heart defects and monitor NT change over time

Between 10 and 12+6 weeks, the fetus roughly doubles in length and becomes about eight times larger in volume.
Only about 1% of fetuses have an NT measurement of ≥3.5 mm (the 99th centile).
With expert ultrasound, around half of major structural anomalies can be detected at 11–14-weeks.
Expert fetal echocardiography at 11–14 weeks can detect over two-thirds of severe congenital heart defects.
We estimate that at least 100 distinct structural conditions are detectable at 12–13 weeks. This is supported by multiple studies showing that around 50% of structural anomalies can be identified between 11 and 14 weeks.
In the case of a high-chance genomic NIPT result, a targeted 12-13 week scan aims to detect structural anomalies and physical differences, trying to refine the prenatal phenotype to guide care.
There are many structural anomalies associated with iNT. The most common include congenital heart defects, spina bifida, congenital diaphragmatic hernia, abdominal wall defects (e.g. exomphalos), renal and bladder anomalies (e.g. urinary tract obstructions), major brain anomalies, and skeletal/limb anomalies. In our experience, a targeted expert scan at 12–13 weeks detects a large proportion of these, because iNT-associated anomalies are often more severe and therefore more visible this early. Conversely, a normal scan together with a improving/normalising NT is strongly reassuring about the baby’s structural integrity.


Learn More about the SMART Protocol
The targeted scan is fundamentally different from a standard 12-week NT scan. Whereas the routine scan focuses on measuring NT and has no protocol for a systematic structural review, SMART NT – Step Two performs a comprehensive assessment of all organs. We also assess tiny structures, like fingers and lips, using a checklist closely modelled on the 20-week anomaly scan. We have over 20 years’ experience with this approach. The scan also measures NT thickness, but uses it to track NT evolution (improving, stable or increasing) rather than as a parameter of the Combined Test.
Learn More about the SMART Protocol
iNT is strongly associated with congenital heart defects (CHD). Early fetal echocardiography (early fetal echo) is an integrated part of our SMART NT - Step Two. It is an ultrasound scan of the fetal heart, a powerful tool that can detect 70-80% of major cardiac anomalies. If iNT reflects an underlying heart problem, it will usually be evident at this stage. Any cardiac findings should prompt referral to a fetal cardiologist for detailed assessment, counselling on likely treatment (often postnatal surgery), and discussion of the long-term outlook.

Learn More about the SMART Protocol
Genotyping means testing the baby’s DNA (e.g. genomic NIPT, CVS, etc) to look for chromosome changes or gene variants (mutations). Phenotyping means assessing the baby’s features on ultrasound (anomalies, structure, growth, “soft markers”, etc) to see how a condition presents and behaves. After a high-chance genomic NIPT result, a targeted 12–13-week ultrasound looks for structural features of the condition and refines prognosis. Some genetic syndromes have recognisable patterns of abnormalities; this scan is designed to identify those features and guide counselling and management.
NT scan and NIPT at 10 weeks, then full results by week 12
1
If increased NT is found, you can have the SMART Test straight away
2
Receive genetic results in 2 weeks
3
Top-to-toe expert fetal examination
Disclaimer! These reflections are my own and arise from practice rather than committee. They do not represent the positions of the FMF, UCLH, NHS, RCOG, ISUOG, or any other organisation. As with any clinician, I may make mistakes or misjudgements. In my view, a carefully performed 10 Week Scan, used alongside appropriately selected modern NIPT and followed by targeted diagnostic testing when indicated, can provide a balanced clinical approach by supporting earlier risk assessment while avoiding unnecessary intervention or over-interpretation. Dr Fred Ushakov
The NT scan is an ultrasound in early pregnancy which measures the thin pocket of fluid at the back of your baby’s neck. This measurement helps estimate the chance of some chromosomal conditions (like Down syndrome) and certain structural problems, especially heart defects.
You lie on the couch and gel is placed on your tummy. The sonographer moves the probe over your abdomen to see the baby on the screen, checks the heartbeat and general development, and then measures the NT at the back of the neck.
Sometimes they need you to cough, wiggle your hips or wait a few minutes for the baby to move into a better position.
It depends on the quality of the ultrasound scanner and the expertise of the operator. Clinics specialising in expert early fetal scans and using state-of-the-art equipment often prefer you to have an empty bladder, as this can actually improve the images for both transabdominal and transvaginal scans.
The traditional approach is different: in early pregnancy a partially full bladder can help lift the uterus and give a clearer view, especially if you have extra weight around your tummy.
Always check the instructions from your own hospital or clinic about whether you should drink beforehand. Many now prefer a “comfortably full” bladder rather than being uncomfortably bursting.
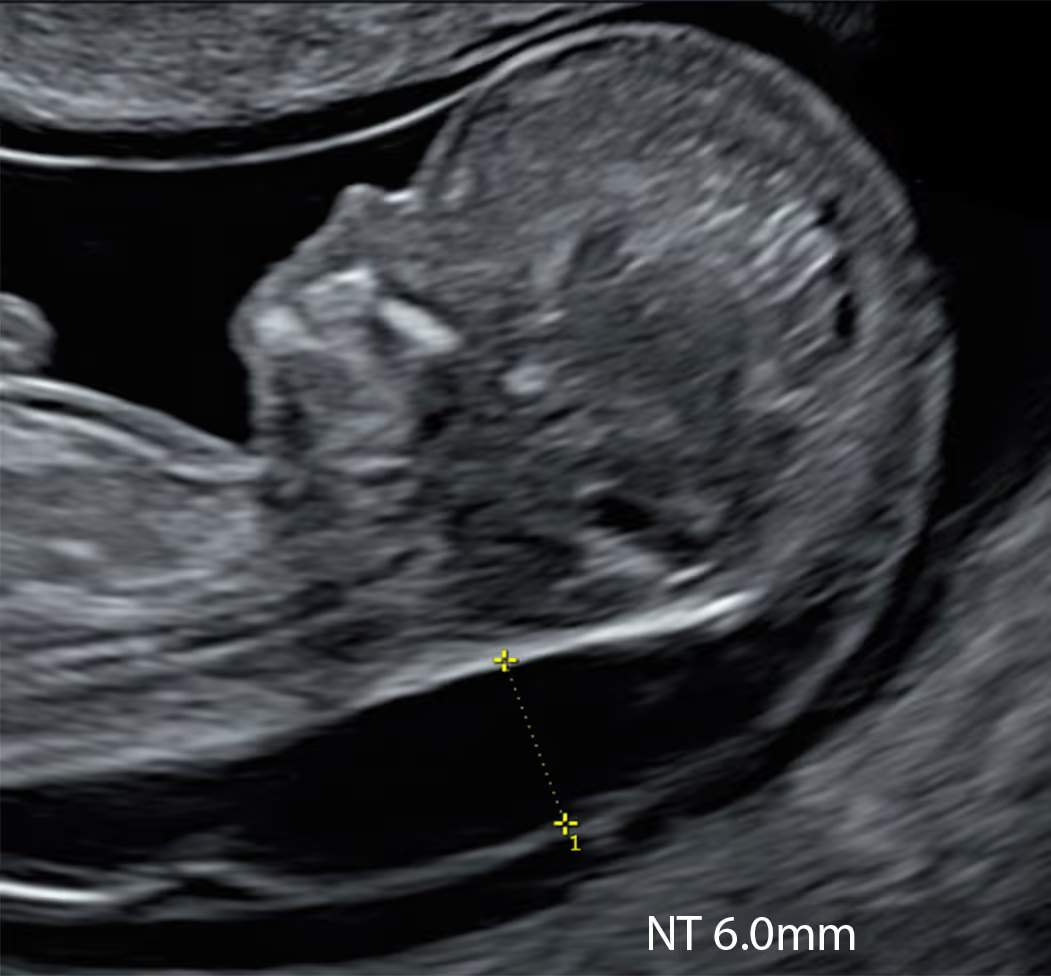
An increased NT means the fluid at the back of the baby’s neck is thicker than expected for that stage of pregnancy. This doesn’t mean there is definitely a problem, but the chance of a chromosomal condition, a heart defect or another underlying issue is higher, so further testing and more detailed scans are normally offered.
You should be offered an appointment with a specialist (for example a fetal medicine doctor or genetic counsellor) to explain the result in detail. The baby should be examined with an special ultrasound scan to check for any structural anomalies, especially heart defects.
You will usually be offered either NIPT (an advanced blood test) or a diagnostic test such as CVS or amniocentesis, plus follow-up ultrasounds, especially to look closely at the baby’s heart and other organs. What you choose is entirely up to you.
It is important to know that, in many countries, the term “high-chance screening result” has now replaced “high-risk screening result.”
Yes. All screening in pregnancy is optional. You can decline the NT scan or blood tests, or choose to have the scan just to see the baby and check dates without having a Combined Screening Test calculation done.
In our view, NT measurement remains crucial because raised NT is closely linked with congenital heart disease. When NT is increased, the baby should be offered a specialist fetal heart scan (fetal echocardiography), so that any heart defect can be detected early and care around birth can be properly planned.
If serious heart problems are not recognised before delivery, the risk of the baby dying soon after birth is much higher.
Yes. All screening in pregnancy is optional. You can decline the NT scan or blood tests, or choose to have the scan just to see the baby and check dates without having a Combined Screening Test calculation done.
In our view, NT measurement remains crucial because raised NT is closely linked with congenital heart disease. When NT is increased, the baby should be offered a specialist fetal heart scan (fetal echocardiography), so that any heart defect can be detected early and care around birth can be properly planned.
If serious heart problems are not recognised before delivery, the risk of the baby dying soon after birth is much higher.
The NT scan is usually done once between 11 and 14 weeks of pregnancy, when your baby measures about 45–84 mm from head to bottom (crown–rump length). After this window the measurement is not reliable.
Recent research, together with our own experience, suggests that the NT scan may actually be more sensitive in the 10-week window, particularly when combined with NIPT. However, this early approach still needs further confirmation in larger studies.
The traditional, and rather limited, view is that the NT scan mainly helps to screen for chromosomal conditions such as Down syndrome (trisomy 21), Edwards syndrome (trisomy 18) and Patau syndrome (trisomy 13).
In reality, a high NT is also strongly linked to serious heart defects, other major structural anomalies and a number of severe genetic syndromes. This means the NT scan should be seen as an important early marker of overall fetal health, helping to guide decisions about further tests and closer follow-up scans.
The cut-off for what is called “increased” NT varies between countries and research groups. Most researchers use the 95th centile as the threshold for increased NT, because this is the standard approach for almost every fetal measurement in medicine. NT also rises naturally as the baby grows, so what is “normal” always depends on your baby’s size.
As a simple rule of thumb, between 11 and 14 weeks an NT under about 3.5 mm is usually considered within the expected range. Measurements of 3.5 mm or more are often labelled “increased” or “high”, but in reality they represent an abnormal NT because they are above the 99th centile. At around 10 weeks’ gestation, the abnormal cut-off is lower, at about 2.5 mm, because the baby is still very small and NT is closely related to fetal size.
Your baby’s result is always interpreted in context, taking into account the exact crown–rump length, gestational age and, where relevant, the associated blood test results.
They do slightly different jobs, so many experts recommend both where available. NIPT is a very accurate blood test for certain chromosomal conditions but cannot check the baby’s structure.
The NT scan looks at the baby’s anatomy, can pick up early physical problems and helps interpret NIPT or combined test results.
The best possible approach is a 10 Week Scan plus NIPT: checking the baby for major structural anomalies, measuring the NT, and taking blood for NIPT all in a single appointment.
This is quite common. The sonographer/doctor may ask you to walk around, have a drink, cough or change position, and then try again. If they still can’t obtain a reliable measurement, you may be rebooked for another day or offered an alternative screening option, such as the second-trimester blood test (the quadruple test).
However, it is important to know that the quadruple test is less effective for screening trisomy 21 (Down syndrome), and up to about 25% of affected babies may be missed (false negative results). For this reason, many professionals will recommend having NIPT if the NT measurement cannot be obtained. NIPT has a detection rate of over 99% for Down’s syndrome.
It depends on the NT cut-off used and the exact stage of pregnancy. Between 11 and 14 weeks, if a cut-off of 3.5 mm (around the 99th centile) is used, roughly 20–30% of fetuses with trisomy 21 (Down syndrome) will still have an NT measurement in the “normal” range.
If a lower cut-off at the 95th centile is used, a larger proportion of fetuses with trisomy 21 will fall into the “increased NT” group. Overall, NT on its own is only a moderate screening tool for trisomy 21, and a normal NT does not rule out Down syndrome.
It depends on the NT cut-off used and the exact stage of pregnancy. Between 11 and 14 weeks, if a cut-off of 3.5 mm (around the 99th centile) is used, roughly 20–30% of fetuses with trisomy 21 (Down syndrome) will still have an NT measurement in the “normal” range.
If a lower cut-off at the 95th centile is used, a larger proportion of fetuses with trisomy 21 will fall into the “increased NT” group. Overall, NT on its own is only a moderate screening tool for trisomy 21, and a normal NT does not rule out Down syndrome.
For medical professionals who want to learn more about the SMART NT approach, access training, and join our clinical network.





