NT: a small measurement with big implications

Discovered in 1992, nuchal translucency or NT remains the key early marker of a baby’s health, supported by more than 3,000 clinical research studies worldwide. It is often combined with other ultrasound markers and blood tests to provide a more accurate assessment of fetal wellbeing.
More than 300 individual genetic variants are thought to be associated with increased NT, representing a broad spectrum of serious fetal conditions. These include chromosomal abnormalities, genetic syndromes, congenital heart defects, and other structural anomalies. Visit our NT Registry page.
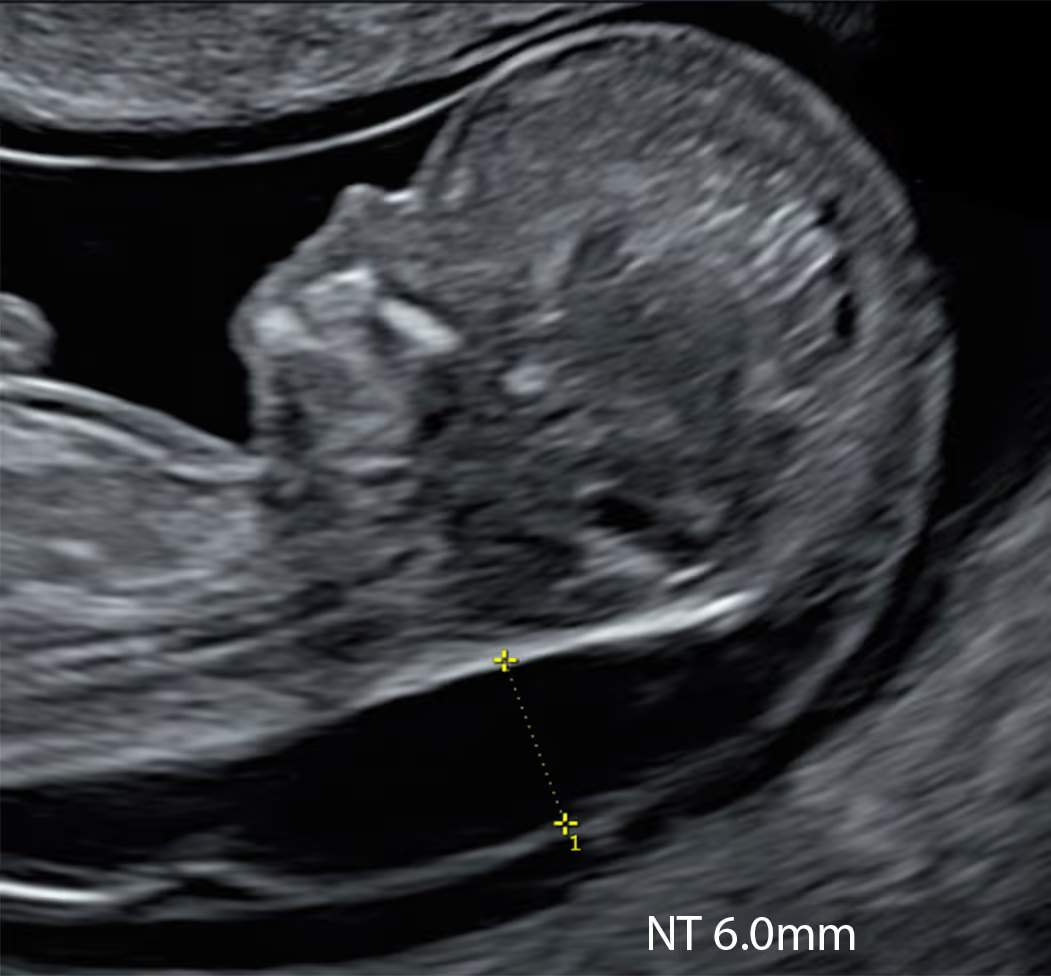
Nuchal translucency (NT) refers to the subcutaneous fluid-filled space between the fetal skin and the soft tissues overlying the cervical spine, visible on ultrasound in the first trimester. A small NT is a normal developmental feature, but an increased NT measurement may indicate chromosomal abnormalities, genetic syndromes, cardiac defects, or other structural anomalies. Assessment of NT provides an important early marker of overall fetal wellbeing.


Learn More about the SMART Protocol
Nuchal translucency (NT) is a small fluid space at the back of the baby’s neck, seen on early ultrasound. Every baby has some fluid, but when the NT is thicker than expected, it can sometimes be an early sign of genetic or structural problems. Measuring NT helps assess the baby’s wellbeing very early in pregnancy. An increased NT does not always mean there is a problem, but it is an important reason to carry out further tests to rule out possible conditions.

Learn More about the SMART Protocol
The NT measurement reflects the early development and balance of fluid within the baby’s tissues and circulation. It depends on the proper function of the heart, blood vessels, and lymphatic system, as well as the composition of the connective tissue. An increased NT may arise from temporary disturbance in fluid balance - for example, due to reduced cardiac function, delayed lymphatic drainage, or changes in tissue fluid permeability. Other biological mechanisms may also contribute, and some remain not yet fully understood.

Learn More about the SMART Protocol
No. An increased NT does not always mean that the baby has a health problem. In some cases, the extra fluid disappears naturally, and the baby develops completely normally. The reason why some healthy babies show an increased NT is not fully understood, but there is strong evidence that when no genetic or structural problems are present, the NT usually resolves and the outcome is good.
Conditions associated with high Nuchal Transluncency (NT)





There are three different periods when nuchal thickness can be measured
At 10 weeks, NT can be measured accurately and may be a more sensitive early sign of possible problems, allowing prompt reassurance or testing.
This is the traditional time for NT assessment as part of the Combined Screening Test (CST). In the UK and many other countries, most babies have their NT measured during this stage of pregnancy.
After 14 weeks, the fluid behind the baby’s neck usually disappears, making the NT measurement unreliable. Instead, a different marker called the nuchal fold (NF) can be measured at this stage.
Increased NT Cut-off day by day chart.
The NT scan is an ultrasound in early pregnancy which measures the thin pocket of fluid at the back of your baby’s neck. This measurement helps estimate the chance of some chromosomal conditions (like Down syndrome) and certain structural problems, especially heart defects.
You lie on the couch and gel is placed on your tummy. The sonographer moves the probe over your abdomen to see the baby on the screen, checks the heartbeat and general development, and then measures the NT at the back of the neck.
Sometimes they need you to cough, wiggle your hips or wait a few minutes for the baby to move into a better position.
It depends on the quality of the ultrasound scanner and the expertise of the operator. Clinics specialising in expert early fetal scans and using state-of-the-art equipment often prefer you to have an empty bladder, as this can actually improve the images for both transabdominal and transvaginal scans.
The traditional approach is different: in early pregnancy a partially full bladder can help lift the uterus and give a clearer view, especially if you have extra weight around your tummy.
Always check the instructions from your own hospital or clinic about whether you should drink beforehand. Many now prefer a “comfortably full” bladder rather than being uncomfortably bursting.
An increased NT means the fluid at the back of the baby’s neck is thicker than expected for that stage of pregnancy. This doesn’t mean there is definitely a problem, but the chance of a chromosomal condition, a heart defect or another underlying issue is higher, so further testing and more detailed scans are normally offered.
You should be offered an appointment with a specialist (for example a fetal medicine doctor or genetic counsellor) to explain the result in detail. The baby should be examined with an special ultrasound scan to check for any structural anomalies, especially heart defects.
You will usually be offered either NIPT (an advanced blood test) or a diagnostic test such as CVS or amniocentesis, plus follow-up ultrasounds, especially to look closely at the baby’s heart and other organs. What you choose is entirely up to you.
It is important to know that, in many countries, the term “high-chance screening result” has now replaced “high-risk screening result.”
Yes. All screening in pregnancy is optional. You can decline the NT scan or blood tests, or choose to have the scan just to see the baby and check dates without having a Combined Screening Test calculation done.
In our view, NT measurement remains crucial because raised NT is closely linked with congenital heart disease. When NT is increased, the baby should be offered a specialist fetal heart scan (fetal echocardiography), so that any heart defect can be detected early and care around birth can be properly planned.
If serious heart problems are not recognised before delivery, the risk of the baby dying soon after birth is much higher.
Yes. All screening in pregnancy is optional. You can decline the NT scan or blood tests, or choose to have the scan just to see the baby and check dates without having a Combined Screening Test calculation done.
In our view, NT measurement remains crucial because raised NT is closely linked with congenital heart disease. When NT is increased, the baby should be offered a specialist fetal heart scan (fetal echocardiography), so that any heart defect can be detected early and care around birth can be properly planned.
If serious heart problems are not recognised before delivery, the risk of the baby dying soon after birth is much higher.
The NT scan is usually done once between 11 and 14 weeks of pregnancy, when your baby measures about 45–84 mm from head to bottom (crown–rump length). After this window the measurement is not reliable.
Recent research, together with our own experience, suggests that the NT scan may actually be more sensitive in the 10-week window, particularly when combined with NIPT. However, this early approach still needs further confirmation in larger studies.
The traditional, and rather limited, view is that the NT scan mainly helps to screen for chromosomal conditions such as Down syndrome (trisomy 21), Edwards syndrome (trisomy 18) and Patau syndrome (trisomy 13).
In reality, a high NT is also strongly linked to serious heart defects, other major structural anomalies and a number of severe genetic syndromes. This means the NT scan should be seen as an important early marker of overall fetal health, helping to guide decisions about further tests and closer follow-up scans.
The cut-off for what is called “increased” NT varies between countries and research groups. Most researchers use the 95th centile as the threshold for increased NT, because this is the standard approach for almost every fetal measurement in medicine. NT also rises naturally as the baby grows, so what is “normal” always depends on your baby’s size.
As a simple rule of thumb, between 11 and 14 weeks an NT under about 3.5 mm is usually considered within the expected range. Measurements of 3.5 mm or more are often labelled “increased” or “high”, but in reality they represent an abnormal NT because they are above the 99th centile. At around 10 weeks’ gestation, the abnormal cut-off is lower, at about 2.5 mm, because the baby is still very small and NT is closely related to fetal size.
Your baby’s result is always interpreted in context, taking into account the exact crown–rump length, gestational age and, where relevant, the associated blood test results.
They do slightly different jobs, so many experts recommend both where available. NIPT is a very accurate blood test for certain chromosomal conditions but cannot check the baby’s structure.
The NT scan looks at the baby’s anatomy, can pick up early physical problems and helps interpret NIPT or combined test results.
The best possible approach is a 10 Week Scan plus NIPT: checking the baby for major structural anomalies, measuring the NT, and taking blood for NIPT all in a single appointment.
This is quite common. The sonographer/doctor may ask you to walk around, have a drink, cough or change position, and then try again. If they still can’t obtain a reliable measurement, you may be rebooked for another day or offered an alternative screening option, such as the second-trimester blood test (the quadruple test).
However, it is important to know that the quadruple test is less effective for screening trisomy 21 (Down syndrome), and up to about 25% of affected babies may be missed (false negative results). For this reason, many professionals will recommend having NIPT if the NT measurement cannot be obtained. NIPT has a detection rate of over 99% for Down’s syndrome.
It depends on the NT cut-off used and the exact stage of pregnancy. Between 11 and 14 weeks, if a cut-off of 3.5 mm (around the 99th centile) is used, roughly 20–30% of fetuses with trisomy 21 (Down syndrome) will still have an NT measurement in the “normal” range.
If a lower cut-off at the 95th centile is used, a larger proportion of fetuses with trisomy 21 will fall into the “increased NT” group. Overall, NT on its own is only a moderate screening tool for trisomy 21, and a normal NT does not rule out Down syndrome.
It depends on the NT cut-off used and the exact stage of pregnancy. Between 11 and 14 weeks, if a cut-off of 3.5 mm (around the 99th centile) is used, roughly 20–30% of fetuses with trisomy 21 (Down syndrome) will still have an NT measurement in the “normal” range.
If a lower cut-off at the 95th centile is used, a larger proportion of fetuses with trisomy 21 will fall into the “increased NT” group. Overall, NT on its own is only a moderate screening tool for trisomy 21, and a normal NT does not rule out Down syndrome.
For medical professionals who want to learn more about the SMART NT approach, access training, and join our clinical network.





