Join the SMART NT network and bring advanced early screening to your patients. We collaborate with selected clinics to provide training, and access to comprehensive genetic testing pathways under the SMART NT program.

While invasive diagnostic testing with CVS or amniocentesis remains the gold standard in pregnancies with increased NT, these tests have important limitations. They do not assess fetal structure and may not detect many monogenic disorders.
State-of-the-art non-invasive investigations can provide additional clinically relevant information without procedure-related risk.
Increased NT, early hydrops, or cystic hygroma? Don’t wait until 12 weeks - refer now for an urgent expert scan, KNOVA NIPT and SMART NT pathway.

Seen early increased NT in your patient and unsure what to do next? Refer her to London Pregnancy Clinic (LPC). LPC offers a robust specialist pathway through its SMART NT protocol.

Join our network through affiliation and SMART NT accreditation: Register your interest today.

Download London Pregnancy Clinic protocol for nuchal translucency measurement at 10 weeks and management of the increased NT

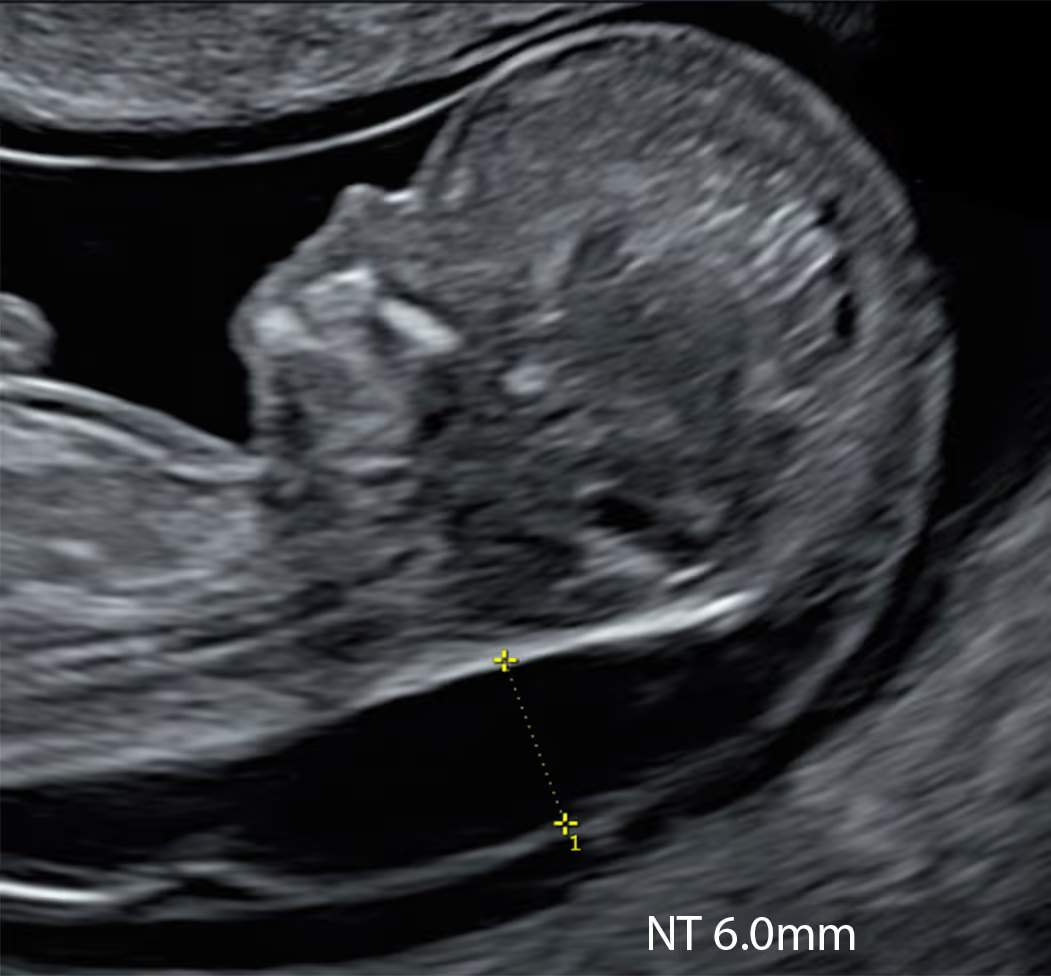
Every practitioner performing early pregnancy scans has encountered a 10-week fetus with a “hydropic appearance” or marked skin oedema. In such situations, professionals often feel frustrated: the baby looks unwell, yet there is no clear pathway for management. The immediate questions are whether to inform the parents and which tests to arrange, or where to refer. It is clear that the CVS option does not exist at 10 weeks. So, should we “ignore” the finding and rescan in two weeks to measure the NT? Does that sound correct?
We have developed the SMART NT protocol: a clear, streamlined 10 weeks NT pathway that combines high-resolution scans with advanced NIPT. Train with us, partner with us, and improve care for pregnant women.
We collaborate with sonographers, obstetricians, early pregnancy or fetal medicine specialists and clinics across both the NHS and private sector. We are equally keen to partner internationally for training, accreditation and rollout.
Based in London, UK, we work with providers delivering first-trimester scanning in any setting. We’re actively seeking global collaborations for training, certification and implementation.
For Greater London providers
If you have a patient at 9–10 weeks with increased nuchal translucency (NT), generalised fetal oedema, cystic hygroma, or early fetal hydrops, please refer her to our clinic for assessment and discussion of the SMART NT pathway. She will receive a discounted 10-week scan as soon as possible (usually within 24–48 hours), discounted KNOVA NIPT, and a targeted scan at 12–13 weeks.
For providers elsewhere in the UK
This pathway may be less practical because of the logistics of travelling to London. We will accept a report from an NHS or other CQC-registered ultrasound provider (an image of the increased NT measurement is essential). We will arrange online NIPT counselling promptly and send a KNOVA kit by courier with instructions. We strongly advise arranging and attending our clinic for the 12–13-week targeted scan.
Please note: the pathway for SMART NT Affiliated Clinics is different.
Early concerns at 9–10 weeks are not limited to increased NT. It’s not uncommon to see a viable fetus at 9–10 weeks with features that look abnormal or unusual, yet there is often no clear UK referral pathway to a Fetal Medicine Unit at this stage. EPAU services are excellent for maternal and gynaecological emergencies and confirming viability, but they are not designed for detailed early fetal anatomical assessment or genetics counselling.
We provide a solution. We offer discounted second-opinion scans led by fetal-medicine specialists, with same- or next-day appointments where possible. We will update you on your patient’s findings and advise on any further actions if required.
You can download our "10 Week NT Measurement and Management Protocol (LPC) - 2025" here.
Starting in 2026, we will launch our free introductory course, Increased NT at 10 Weeks: Diagnosis, Management and Prognosis.
We will then introduce our advanced training module, Encyclopaedia of Early Anomalies
This will be followed by a formal certification and affiliation programme.
Disclaimer! These reflections are my own and arise from practice rather than committee. They do not represent the positions of the FMF, UCLH, NHS, RCOG, ISUOG, or any other organisation. As with any clinician, I may make mistakes or misjudgements. But I believe that coupling a careful 10 Week Scan with modern NIPT, and escalating to targeted diagnostics when indicated, offers families the balance we seek: early clarity without haste, and precision without noise.
We plan to launch our free introductory online course, Increased NT at 10 Weeks: Diagnosis, Management and Prognosis, in autumn 2026. Register your interest to receive updates about the exact course launch date, the programme, and future educational activities.
KNOVA NIPT may not currently be available in every country, and access can vary depending on local regulations, sample collection arrangements, shipping requirements and customs rules. A practical first step is to contact a genetics provider such as Jeen (jeen.health) and ask whether KNOVA can be arranged in your country. Jeen states that KNOVA is available across the UK and in some EU regions, and that testing can be organised either through a self-arranged blood draw or through participating clinics. Jeen also states that KNOVA can be performed from 10 weeks, with a typical laboratory turnaround time of 7 to 10 working days from receipt of the sample.
For patients with increased NT, it is often preferable to work with a provider specialising in both fetal ultrasound and genomics, so that the pathway can be coordinated properly. London Pregnancy Clinic (LPC) has experience with KNOVA testing and also sees international patients. LPC states that patients do not need to be registered with the NHS to have screening there, and that results can be communicated to an overseas healthcare provider. LPC also emphasises that NIPT should be combined with expert ultrasound, because NIPT cannot detect structural abnormalities such as heart or brain defects. Their team notes that some severe fetal anomalies may be detectable as early as 10 weeks, which is why a specialist scan is an important first step for pregnancies with increased NT.
This is important because, in a pregnancy with increased NT, a specialist scan may identify structural findings that change the counselling, clarify the level of risk, or influence whether further diagnostic testing should be considered. If the scan is reassuring, KNOVA may then serve as an additional screening option for severe genetic conditions. If the patient is travelling from abroad, working with an experienced centre may also make the process smoother by helping to coordinate the scan, blood sampling, reporting and communication with the patient’s local doctor. Even so, cross-border testing can still be affected by practical issues such as local phlebotomy arrangements, transport logistics and country-specific import rules, so it is always sensible to confirm feasibility in advance.
Our formal theoretical programme on the 10 Week Scan and NIPT approach is currently in development, with the aim of providing a structured introduction to the principles, clinical pathway, case selection, counselling, interpretation of findings, and follow-up management.
In addition, observational experience at London Pregnancy Clinic (LPC) may also be possible and can be discussed on an individual basis. This can be particularly valuable for clinicians who want to see how the pathway works in real clinical practice, including early ultrasound assessment, decision-making, and integration with genomic testing.
If you are interested, the LPC management would be happy to discuss your background, level of experience, and what type of training or observation would be most useful for you.
SMART NT Affiliated Clinic is a clinic connected to the SMART NT professional network, dedicated to advancing care for pregnancies with increased nuchal translucency. Affiliation reflects a strong interest in the SMART NT approach, including early expert ultrasound, advanced prenatal genomic screening, and structured follow-up pathways.
It also offers valuable opportunities for training, education, collaboration, and professional support, including access to a wider network of clinicians who can help with challenging and complex cases. In this way, a SMART NT Affiliated Clinic becomes part of an international effort to raise standards, share expertise, and improve care for families facing increased NT.
Contact us today to find out more and register your interest.
No, absolutely not. We do not have any financial relationship with Fulgent other than using their genomic services in clinical practice. We also work with multiple laboratories in different countries and aim to remain objective in our recommendations.
The clinical reason why KNOVA NIPT has been selected as the main NIPT we currently advise in cases of increased NT is straightforward. At present, KNOVA offers the most balanced panel for this specific indication, including assessment for a wide range of monogenic conditions known to be associated with increased NT. It also has a very low no-call rate, reported to be less than 1%.
We strongly believe that competition between genetic companies is important and ultimately benefits patients and clinicians. It is entirely possible that other laboratories will develop better NIPT options in the future. We continuously review developments in prenatal genomics and reassess the available evidence. If another test proves to be better suited for this clinical scenario, we would be fully prepared to update our SMART NT pathway accordingly.
We currently have experience only with GE Voluson systems, including both the Expert and Signature series. For that reason, we cannot give specific recommendations regarding other ultrasound vendors, as we do not have direct hands-on experience with them. That said, we recognise that several other manufacturers are also capable of producing high-quality imaging.
For the transabdominal 10 Week Scan, we mainly use the microconvex C2-9 probe and, in some cases, the 9L linear probe, provided that the machine settings are well optimised.
For transvaginal scanning, we use only 3D probes. Our preferred option is the RIC 6-12-D, which offers excellent resolution, although its penetration can be limited and it may be less suitable in technically difficult examinations. The RIC 5-9-D is also a very good and reliable option. The newer RIC 10-D appears to offer a good balance between resolution and penetration.
To assess a fetus measuring only 3–4 cm, you need an ultrasound system with very high spatial resolution. A premium system is ideal, and high-end consoles are generally preferable, although some good mid-range platforms may also be suitable if image quality and probe performance are strong enough. A system with dedicated OB/GYN applications is strongly preferable.
Probes are critically important. For the main transabdominal examination, the preferred probe is usually a high-frequency microconvex transducer or, in selected situations, a high-frequency linear probe, ideally in the 7.5–10 MHz range. These can provide the level of detail needed for the 10 Week Scan.
For the transvaginal examination, we believe that 3D/4D capability is essential for clinical work at 10 weeks, so the transvaginal probe should be a 3D/4D probe. Frequencies in the 10–12 MHz range are preferable, as they provide better resolution for early fetal anatomy assessment.
Finally, machine tuning and preset optimisation are extremely important. Even good equipment may underperform if the settings are not properly adjusted, while a well-optimised system can make a major difference to image quality and diagnostic confidence during the 10 Week Scan.
The NT criteria used at 10 weeks differ from the FMF and NHS criteria because the standard FMF/NHS rules were designed for a later stage of the first trimester, when the fetal CRL is 45–84 mm. At 10 weeks, the fetus is smaller and anatomically less mature, so the same measurement framework cannot be applied in exactly the same way.
The SMART NT approach therefore uses dedicated 10-week criteria for fetuses with CRL below 45 mm, before reverting to standard FMF criteria once the fetus reaches the official range. These criteria are based on published evidence showing that increased NT before 11 weeks is a clinically important finding associated with a significant risk of adverse outcome. At the same time, they should be understood as part of the SMART NT clinical approach, rather than as official FMF or NHS guidance.
LPC is a principal private provider of advanced first-trimester ultrasound in London and the UK. It has developed a distinctive 10 Week Scan and NIPT approach, designed to bring together very early detailed ultrasound assessment with appropriately selected prenatal genomic screening. LPC has extensive experience with different types of NIPT, including their strengths, limitations, and role within the wider clinical pathway. Its work also includes the assessment and management of pregnancies with early ultrasound abnormalities, including increased NT, and the integration of imaging with genetic counselling and follow-up testing.
For your practice, LPC’s experience may be relevant in several ways: it can help inform earlier risk assessment, improve understanding of how to combine ultrasound and NIPT effectively, and support more structured counselling and referral pathways for complex first-trimester cases.
Never. In fact, we ask patients to attend with an empty bladder.
A full bladder can push the uterus away from the suprapubic area, which is the part of the abdomen with the thinnest subcutaneous tissue layer. During the transabdominal scan, this can reduce image resolution.
An overfilled bladder may also lead to contraction of the isthmic part of the uterus after the patient empties it. This contraction can significantly interfere with transvaginal imaging.
A full bladder is also simply uncomfortable for patients and can become an unnecessary distraction during the examination, especially when careful attention and good cooperation are important.
In summary, we ask women to empty their bladder before the 10 Week Scan.
For medical professionals who want to learn more about the SMART NT approach, access training, and join our clinical network.

Lorem ipsum dolor sit amet conse ctetur adip iscing elit justo quis odio sit sit ac port titor sit males dolor sit consectur dolor.

Lorem ipsum dolor sit amet conse ctetur adip iscing elit justo quis odio sit sit ac port titor sit males dolor sit consectur dolor.

Lorem ipsum dolor sit amet conse ctetur adip iscing elit justo quis odio sit sit ac port titor sit males dolor sit consectur dolor.

Lorem ipsum dolor sit amet conse ctetur adip iscing elit justo quis odio sit sit ac port titor sit males dolor sit consectur dolor.

Lorem ipsum dolor sit amet conse ctetur adip iscing elit justo quis odio sit sit ac port titor sit males dolor sit consectur dolor.

Lorem ipsum dolor sit amet conse ctetur adip iscing elit justo quis odio sit sit ac port titor sit males dolor sit consectur dolor.





