Basic or standard NIPT: screens for Down syndrome (T21), Edwards syndrome (T18) and Patau syndrome (T13)

Current NIPT options provide very high screening accuracy for trisomy 21 (Down syndrome)
NIPT performance for trisomy 18 is strong, though typically not quite as accurate as for trisomy 21
NIPT performance for trisomy 13 is good, but it is typically lower than for trisomy 21 (and usually lower than for trisomy 18)
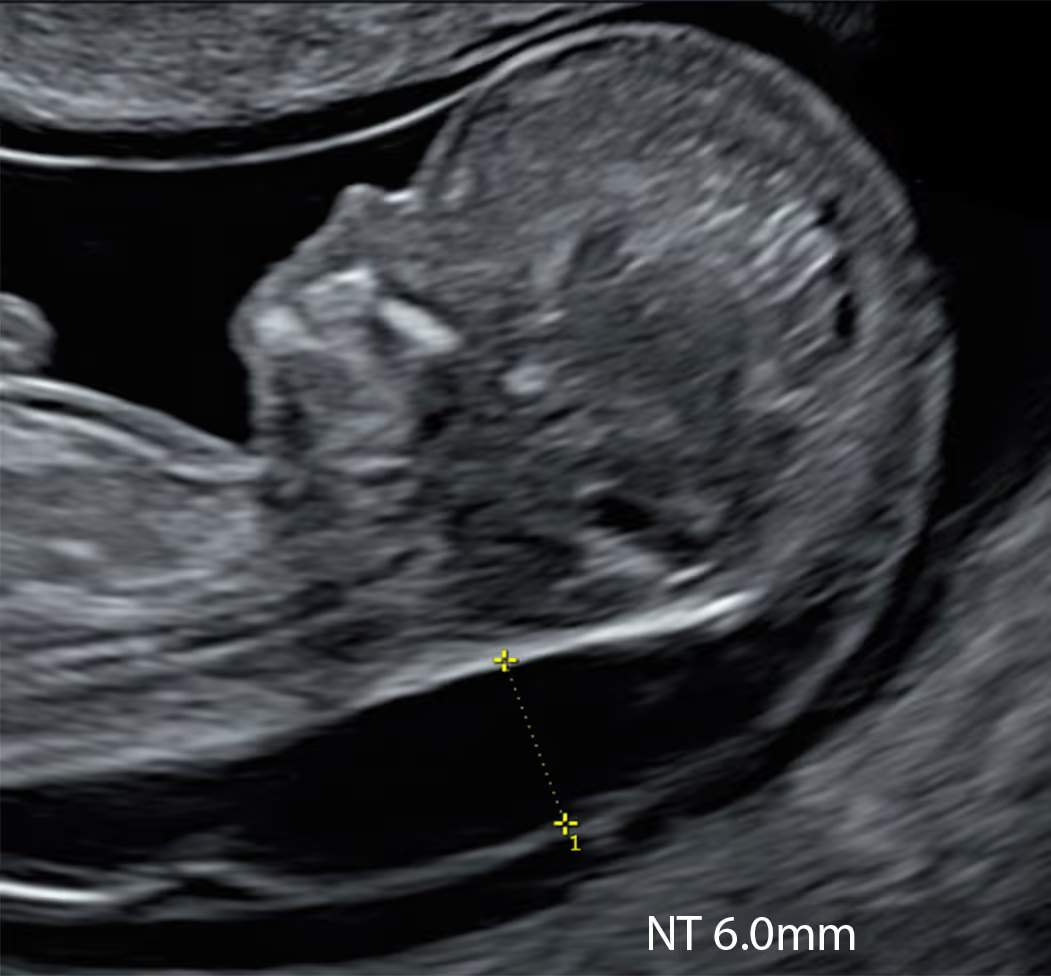
Importantly, basic NIPT does not screen for the many other genetic and chromosomal conditions (around 300) that may be associated with increased NT
Basic NIPT is a useful test in the case of increased NT; however, it is not a perfect one. It screens for some of the most common associations with increased NT: Down syndrome (trisomy 21), Edward syndrome (trisomy 18) and Patau syndrome (trisomy 13), but it does not check for many other chromosomal and genetic associations. NIPT does not detect structural anomalies (including heart defects); that’s the role of ultrasound.
It offers very high sensitivity for trisomies 21, 18 and 13, reducing - but not eliminating - the chance of those conditions (rare false negatives can occur). It doesn’t cover monogenic disorders (such as Noonan syndrome) or microdeletions (such as DiGeorge syndrome). The majority of basic NIPTs do not cover Turner syndrome (monosomy X), which is commonly associated with severely increased NT. It’s a screening, not diagnostic, test, and high-chance results will need confirmation by CVS or amniocentesis.
In the increased-NT scenario, use it alongside a targeted scan; based on findings, consider genomic NIPT or proceed to diagnostic testing (CVS from 11 weeks).
Numerous brand names exist for essentially the same screening test for common chromosomal conditions, which we recognise is confusing. The leading brands include:
BBSafe (Cerba HealthCare, France), Claria (MedGenome, India), Generation (Genomic Diagnostics/Sonic Healthcare, Australia), Harmony (Ariosa Diagnostics/Roche, United States), IONA (Yourgene Health, United Kingdom), MaterniT21 (Labcorp/Sequenom, United States), myPrenatal (Veritas Intercontinental, Spain), NACE (Igenomix, Spain), neoBona (SYNLAB, Germany), NIFTY (BGI Genomics, China), Panorama (Natera, United States), Percept (VCGS, Australia), PrenaTest (LifeCodexx, Germany), Prequel (Myriad Genetics, United States), Prenatal-CODE (GeneticLab, Argentina), PrenatalSafe (Eurofins Genoma, Italy), QNatal Advanced (Quest Diagnostics, United States), SAFE T21 Express (Xcelom, Hong Kong, China), SAFE test (Yourgene Health, United Kingdom), SANCO (Genomed, Poland), Tranquility (Genoma, Italy), UNITY (BillionToOne, United States), Vanadis NIPT (Revvity, United States), Veracity (NIPD Genetics/Medicover Genetics, Cyprus), Verifi (Illumina, United States), VeriSeq NIPT (Illumina, United States).
Many brands are traded internationally and may be run in partner or daughter laboratories in other countries. The same brand name can therefore refer to different physical labs.
No definitive, independent, multi-brand head-to-head study exists. Moreover, the same brand may not perform identically everywhere. Labs may use different technologies (e.g. SNP-based, counting/NGS, rolling-circle), instruments, kit versions and bioinformatics pipelines. Local quality control, fetal-fraction thresholds and reporting rules also vary so reliability can differ by lab.
In practice, large antenatal providers who use several NIPT brands simultaneously often know the real-world performance from their internal audits (e.g. no-call rates, PPV, redraw success), which can be very informative.
Basic NIPT is recommended for all pregnant women, regardless of age or baseline risk. Trisomy 21 is relatively common - 1 in 331 pregnancies according to England and Wales Register, (NCARDRS Data for 2022), and the Combined Screening Test (CST) can miss about 10–15% of cases; basic NIPT therefore offers a significant degree of reassurance.
However, when NT is increased, basic NIPT has limited scope because it does not cover many associated conditions; a targeted early anomaly scan with genomic NIPT (extended panel) or diagnostic testing (CVS from 11 weeks) are generally preferable.
Don’t choose in isolation. Work with a large antenatal provider that specialises in prenatal screening and has genetics and expert ultrasound on site. Such centres usually (1) hold internal audit data across multiple NIPT brands (real-world no-call rates, NPV, PPV, redraw success), (2) use accredited labs (e.g. ISO 15189/CLIA/UKAS), and (3) have clear pathways for high-chance results (rapid fetal medicine referral, CVS/amnio, fetal cardiology, counselling).
What to ask before you decide:
Caution: Smaller providers may list multiple NIPT brands yet lack insight into real-world performance, rely on non-accredited labs, and have limited genetics support and follow-up - reducing overall reliability.
Disclaimer! These reflections are my own and arise from practice rather than committee. They do not represent the positions of the FMF, UCLH, NHS, RCOG, ISUOG, or any other organisation. As with any clinician, I may make mistakes or misjudgements. But I believe that coupling a careful 10 Week Scan with modern NIPT, and escalating to targeted diagnostics when indicated, offers families the balance we seek: early clarity without haste, and precision without noise.
Basic NIPT screens mainly for the three most common chromosome conditions: Down syndrome (trisomy 21), Edwards syndrome (trisomy 18), and Patau syndrome (trisomy 13). Advanced NIPT includes these and may also screen for sex chromosome conditions (such as Turner or Klinefelter syndromes), and usualy for selected microdeletions (small missing pieces of chromosomes). It can also report the baby’s biological sex with high accuracy if you choose to know (and it can be omitted if you prefer not to).
The most comprehensive “extended” NIPT options (for example KNOVA by Fulgent) can additionally screen for a panel of single-gene (monogenic) conditions. This can be particularly relevant when the baby has an increased nuchal translucency (NT), because a meaningful proportion of increased-NT cases are linked to monogenic syndromes (for example RASopathies and certain skeletal or other severe genetic conditions). Importantly, even after CVS/amnio, monogenic testing is not always included unless it is specifically requested, so extended NIPT may help highlight conditions that would otherwise not have been assessed.
Because the scope varies widely between brands and panels, it’s essential to check exactly what your chosen NIPT does and does not screen for, and to interpret the result alongside a high-quality ultrasound scan.
Unlike some European countries such as the Netherlands and Belgium, the NHS screening pathway in England does not currently offer NIPT as a first-line test to everyone. Instead, most people are first offered the combined screening test (CST) in the first trimester (or the quadruple test later on), and only if that result is higher chance is contingent NHS NIPT offered.
When NHS NIPT is offered through this pathway, it is a basic NIPT that screens only for trisomy 21 (Down syndrome), trisomy 18 (Edwards syndrome) and trisomy 13 (Patau syndrome) - it does not screen for other chromosomal conditions, microdeletions and monogenic disorders and it does not report fetal sex within the NHS programme.
Different NHS genomic laboratories (and sometimes contracted providers) deliver the service, so the laboratory platform, turnaround times and report format can vary slightly, but the scope of screening (T21/T18/T13 only) is standard nationwide within the NHS screening programme.
The NHS relies on three genomic laboratory hubs (GLH) for its Non‑Invasive Prenatal Testing (NIPT) service: St George’s SAFE laboratory (South East GLH), the West Midlands Regional Genetics Laboratory (Central & South GLH), and Health Services Laboratories (North Thames GLH). These laboratories are UKAS‑accredited, ensuring high standards.
The NIPT technology varies between labs. Each uses next‑generation sequencing, but the platforms differ - St George’s employs the IONA Nx workflow, the West Midlands uses Illumina’s VeriSeq NIPT LRM module on a NextSeq 550, and HSL utilises Illumina’s VeriSeq NIPT Solution v2.
Most high-quality studies show NIPT detects about 99% (or slightly more) of trisomy 21 pregnancies, which translates to a false-negative rate of roughly about 1% among pregnancies that truly have trisomy 21. In real-life practice, the miss rate is often quoted as lower than that (closer to a few per thousand), but it varies by test platform, laboratory thresholds, and the population being tested.
False negatives can happen for reasons such as low fetal fraction, true fetal mosaicism (the placenta’s DNA is normal, however the baby is affected), or technical/sample issues. So a “low chance” result is very reassuring for trisomy 21, but it is not a guarantee; if you have a strong ultrasound concern (such as markedly increased NT or major anomalies), diagnostic testing is the only way to be certain.
You can usually have NIPT from 10 weeks of pregnancy. Some laboratories may offer testing from 9 weeks, but the chance of a “no result” (no-call) can be higher that early because there may be less placental DNA in the blood sample. For safety and accurate interpretation, we recommend a pregnancy scan before the blood test.
The scan is important to: confirm the pregnancy is viable, date the pregnancy accurately, and check whether there is one baby or twins (as this affects which tests are suitable and how results are interpreted). It can also identify factors such as a vanishing twin, bleeding, or an unexpectedly earlier gestation, all of which can influence test reliability and result interpretation.
Ideally, the scan also includes an early review of anatomy (as far as is possible at that gestation), because ultrasound can detect structural problems that NIPT cannot.
Yes - NIPT is very safe for you and your baby. It is a non-invasive blood test taken from your arm, with no physical contact with the baby, and it does not increase the risk of miscarriage. This is different from invasive diagnostic tests such as CVS or amniocentesis, which involve taking a sample from the pregnancy and carry a small miscarriage risk.
NIPT is very accurate for the common trisomies, particularly Down syndrome (trisomy 21). Large meta-analyses report detection (sensitivity) of about 99% for trisomy 21, around 97% for Edwards syndrome (trisomy 18), and high detection for Patau syndrome (trisomy 13) (often quoted in the ~90–97% range depending on the dataset and platform).
Compared with the standard Combined Screening Test (CST), NIPT has a much lower false-positive rate (specificity typically ~99.9% in pooled analyses), meaning far fewer people are told they are “high chance” when the baby is actually unaffected. In practical terms, that translates into fewer unnecessary referrals and fewer invasive tests (CVS or amniocentesis) prompted by false alarms - while still remembering that NIPT remains a screening test, not a diagnosis.
Yes, definitely. Even “basic” NIPT is a sophisticated genetic screening test, and it can sometimes lead to results that need careful explanation, such as a high-chance result, a no-call/no result, or an unexpected/atypical finding (for example findings that may be related to the placenta or, rarely, the mother rather than the baby).
Good counselling makes sure you understand exactly what the test is looking for, what it cannot detect, and what choices you may face depending on the result.
Pre-test counselling should cover the scope of the test, its accuracy, and its limitations (including the fact it is a screening test, not a diagnosis). It should also explain the next steps if the result is high chance or unclear - for example, whether you would consider diagnostic testing (CVS or amniocentesis), and what extra ultrasound follow-up might be recommended.
This is particularly important if you have an increased NT or any other scan finding, because interpretation and follow-up need to be planned properly.
Counselling can be provided by appropriately trained professionals such as doctors, midwives, sonographers, or a qualified genetic counsellor. It’s also a chance to discuss practical points such as timing, turnaround time, what happens if there is a redraw, and whether you want to know the baby’s sex (if that is offered).
Most importantly, it gives you space to ask questions and make a decision that feels right for you and your family.
Yes, definitely. Even “basic” NIPT is a sophisticated genetic screening test, and it can sometimes lead to results that need careful explanation, such as a high-chance result, a no-call/no result, or an unexpected/atypical finding (for example findings that may be related to the placenta or, rarely, the mother rather than the baby).
Good counselling makes sure you understand exactly what the test is looking for, what it cannot detect, and what choices you may face depending on the result.
Pre-test counselling should cover the scope of the test, its accuracy, and its limitations (including the fact it is a screening test, not a diagnosis). It should also explain the next steps if the result is high chance or unclear - for example, whether you would consider diagnostic testing (CVS or amniocentesis), and what extra ultrasound follow-up might be recommended.
This is particularly important if you have an increased NT or any other scan finding, because interpretation and follow-up need to be planned properly.
Counselling can be provided by appropriately trained professionals such as doctors, midwives, sonographers, or a qualified genetic counsellor. It’s also a chance to discuss practical points such as timing, turnaround time, what happens if there is a redraw, and whether you want to know the baby’s sex (if that is offered).
Most importantly, it gives you space to ask questions and make a decision that feels right for you and your family.
NIPT gives you a safe and early look at your baby’s health, explore the conditions we can screen for during pregnancy.
A highly accurate NIPT that screens for common and rare genetic conditions in your baby – including microdeletions.

Comprehensive blood tests for cancer markers, helping detect risks early with results guided by medical specialists.

Advanced NIPT available for single or twin pregnancies, egg donors and IVF. Optional panels for microdeletions and rare syndromes.

A cost-effective, high-quality NIPT that screens for common conditions and can include testing for inherited conditions.

For medical professionals who want to learn more about the SMART NT approach, access training, and join our clinical network.





