SMART NT Step One:
Combining the earliest structural screening for most severe anomalies with precise NT measurement in a single scan

At 10 weeks, the fetus is usually about 30–40 mm (CRL), roughly the size of a strawberry or a small apricot.
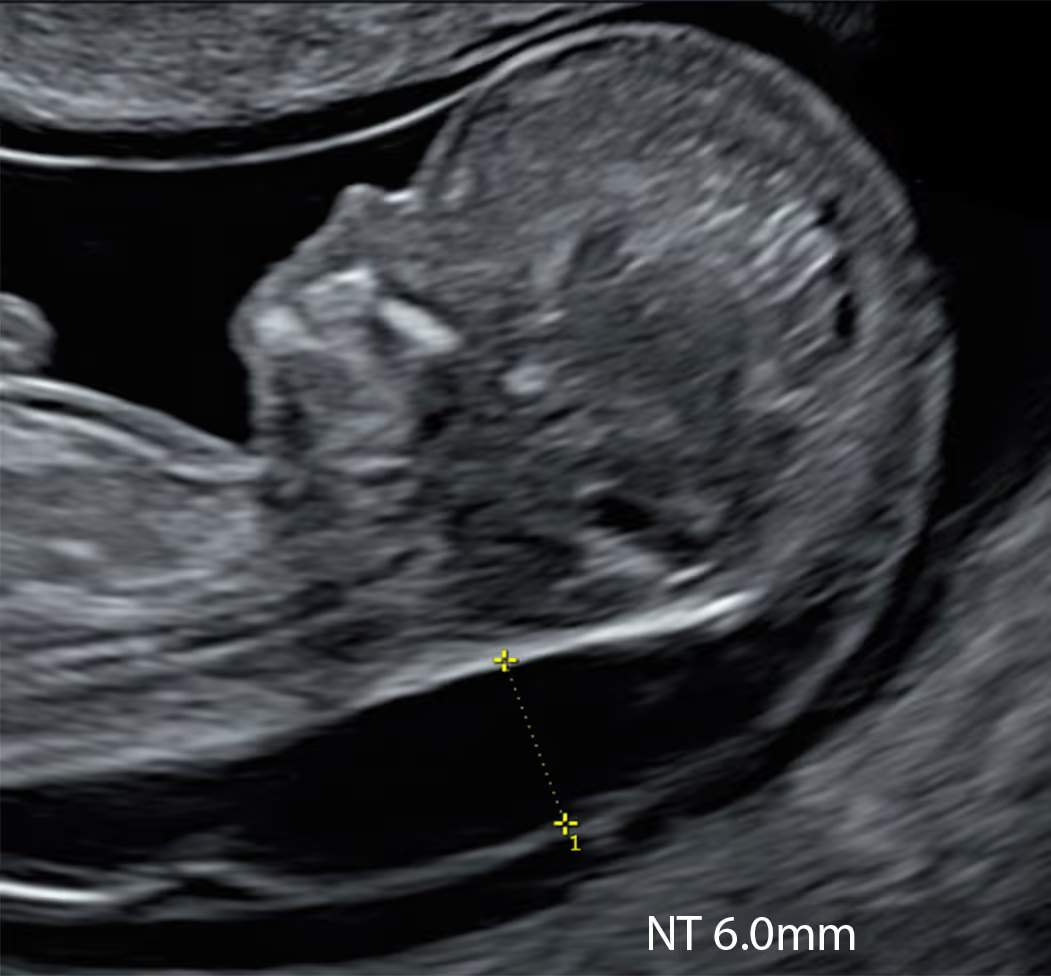
At 10 weeks, an NT measurement of ≥2.5 mm is considered abnormal and, is associated with an ~40% chance of an adverse pregnancy outcome.
Acrania, alobar holoprosencephaly, spina bifida, absence of arms/legs, encephalocele, omphalocele with liver, amniotic band syndrome, body stalk anomaly, sirenomelia, cloacal exstrophy.
In normal pregnancies, fetal heart rate (FHR) peaks around 9–10 weeks at about ~170 bpm (often roughly 160–180 bpm)
One-stop 10 Week Scan + NIPT. If iNT (NT ≥2.5 mm; CRL <45mm) is found, we recommend proceeding with KNOVA. If NT is normal, KNOVA is optional; we advise to discuss basic versus advanced NIPT and choose according to context and preference.
Apart from measuring NT, the 10-week scan can reveal lethal non-genetic anomalies and features suggestive of a genetic condition. Lethal non-genetic anomalies are NIPT exclusion criteria; when findings suggest a genetic cause, KNOVA is the preferred screen.
According to recent data, an NT measurement of 2.5 mm or greater at 10 weeks is associated with an abnormal fetal outcome in about 42% of cases. This cut-off has been adopted in our protocol, and any measurement at or above this level triggers the SMART NT pathway. It is important to note that this value is higher than the 95th centile for this stage of pregnancy, which is typically 2.1–2.4 mm.


Learn More about the SMART Protocol
Alobar holoprosencephaly, heart defects, limb abnormalities, exomphalos with liver, and particularly early fetal hydrops or cystic hygroma are strongly associated with chromosomal or genetic syndromes. At later stages, these findings usually warrant diagnostic testing (CVS); however, CVS cannot be performed safely at 10 weeks. In such cases, we recommend starting with a genomic NIPT as the first step. A high-chance NIPT result, especially for monogenic conditions, can help guide the planning of further diagnostic tests.

Learn More about the SMART Protocol
Acrania, body stalk anomaly, cloacal exstrophy, pentalogy of Cantrell, sirenomelia, amniotic band syndrome, and limb–body–wall complex are usually NOT associated with genetic conditions. Most of these anomalies are lethal or have an extremely poor outcome. If such conditions are detected at 10 weeks, we strongly recommend NOT proceeding with NIPT, as performing it may delay appropriate referral and management, and a low-risk result could provide false reassurance.

Learn More about the SMART Protocol
The SMART NT protocol cannot be used in certain situations where genomic NIPT (KNOVA) is not applicable. These include early not genetic fetal anomalies, twin or triplet pregnancies, vanishing twin, donor egg IVF pregnancies. Maternal ineligibility includes cases where the mother has a history of recent cancer, organ or bone marrow transplantation. In such cases, the fetal cfDNA in the mother’s blood cannot be accurately analysed, making genomic NIPT unreliable.
A 10 Week Scan is a detailed ultrasound examination performed at around 10 weeks of pregnancy to assess the baby’s early development. Although the fetus is still very small, many important structures can already be seen, including the early brain, spine, abdominal wall, limbs and heart position. In our view, with modern high-resolution ultrasound and advanced NIPT, the 10 Week Scan has the potential to become the main early screening scan and may eventually replace the traditional 12–13-week screening scan. At present, however, a targeted follow-up scan at 12–13 weeks remains important in selected cases, especially when NT is increased or early anatomy is not completely reassuring.
The 10 Week Scan is different from the standard 12 Week Scan because it is performed earlier, usually by transvaginal ultrasound, which can provide higher resolution than a standard 12-week transabdominal scan. This allows very detailed assessment of early fetal anatomy, including the brain, spine, abdominal wall, limbs, heart position and NT, at a stage when many important developmental features can already be seen. In our experience, 10 weeks is also the best time to use diagnostic 3D ultrasound, as the fetus is small enough to acquire high-quality 3D volumes for detailed review and audit. Currently the 12 Week Scan remains standard first-trimester ultrasound, but the 10 Week Scan can provide earlier reassurance, earlier detection of significant problems and better integration with NIPT.
At the 10 Week Scan, many key fetal structures can already be assessed reliably, especially when high-resolution transvaginal ultrasound and 3D imaging are used. This includes the early brain, skull, spine, abdominal wall, stomach, bladder, cord insertion, limbs, hands and feet, fetal movements, heart position and basic cardiac activity. NT can also be assessed at this stage and is one of the most important early markers of fetal health. Some structures are still very small or immature, so the 10 Week Scan should be seen as an early detailed assessment rather than a complete replacement for all later anatomical checks.
At the 10 Week Scan, we can potentially detect a range of major structural abnormalities, particularly those affecting the brain, skull, spine, abdominal wall, limbs, bladder and early heart position. Examples include severe brain (alobar holoprosencephaly)and skull (acrania) abnormalities, major spinal defects, large abdominal wall defects, abnormal limb development, severe bladder enlargement, increased NT, early hydrops and some major cardiac or body-position abnormalities. The scan can also identify findings that may suggest a higher risk of genetic or syndromic conditions, even when NIPT is low risk. However, understandably not all abnormalities are visible at 10 weeks, and some develop or become clearer later in pregnancy, so follow-up imaging is strongly recommended.
The best approach is to use both — starting with a transabdominal scan (TAS) and then offering a transvaginal scan (TVS) for a more detailed assessment.
We begin with TAS. No full bladder is needed, and in most cases TAS provides excellent diagnostic images to confirm the number of babies, document the heartbeat, observe fetal movements, and measure the crown–rump length (CRL). In many pregnancies, TAS is also preferred for measuring the NT at 10 weeks because, due to gravity, the baby often lies on its back, which can make the mid-sagittal view easier to obtain.
TAS can give a useful overview of early fetal anatomy, but a precise, structured assessment of fetal structures at 10 weeks is usually better with TVS. Once we have obtained as much information as possible abdominally, we offer TVS. In our experience, most patients choose to proceed, as TVS typically provides the highest-resolution views for early anatomy and can also help with NT measurement when the fetal position is optimal.
If the baby’s position is not suitable for a direct NT measurement (for example, an oblique or coronal view), there is also the option of using a reconstructed 3D dataset to obtain an accurate measurement.
The main limitation of the 10 Week Scan is that the fetus is still very small and some organs are not yet fully developed or easy to assess. Even with high-resolution transvaginal ultrasound and 3D imaging, not every abnormality can be seen at this stage. Some problems, especially more subtle heart, brain, kidney, facial, skeletal or growth-related abnormalities, may only become visible later in pregnancy. Image quality can also be affected by fetal position, maternal anatomy, fibroids, bleeding, or technical factors. Therefore, a normal 10 Week Scan is very reassuring, but it cannot guarantee that the baby has no structural or genetic condition, and follow-up scans are needed.
High-resolution ultrasound is especially important at 10 weeks because the fetus is still very small and even tiny anatomical details matter. Better image resolution allows the sonographer to see early structures more clearly, measure NT more accurately and identify subtle findings that may be missed with lower-quality imaging. Transvaginal ultrasound often provides excellent resolution at this stage, and diagnostic 3D can also be very helpful for reviewing the fetal anatomy in detail. Without high-resolution equipment and specialist experience, a 10 Week Scan can easily become unreliable or falsely reassuring.
The 10 Week Scan and NIPT work very well together because they check different things. NIPT is highly effective for screening the most common chromosomal conditions, such as Down syndrome, Edwards syndrome and Patau syndrome, but it cannot assess the baby’s anatomy. The 10 Week Scan adds an early structural assessment, including NT, brain, spine, abdominal wall, limbs, early heart position and other key developmental features. This means that NIPT can provide powerful genetic screening, while the scan can identify structural findings or increased NT that may suggest the need for extended NIPT, diagnostic testing or targeted follow-up imaging. Together, they give earlier and broader information than either test alone.
Yes. NIPT is excellent for screening selected chromosomal conditions, especially Down syndrome, Edwards syndrome and Patau syndrome, but it cannot examine the baby’s anatomy. American College of Obstetricians and Gynecologists specifically notes that structural defects may occur with or without aneuploidy, which is why ultrasound assessment remains important even when cfDNA/NIPT is low risk.
The 10 Week Scan can potentially detect problems that NIPT may miss, such as major brain or skull abnormalities, spinal defects, abdominal wall defects, limb abnormalities, abnormal early heart position, hydrops and increased NT. Some of these findings may also be early signs of genetic or monogenic conditions that are not covered by basic NIPT panels. NHS Genomics also states that NIPT is not designed to detect fetal genetic conditions outside the targeted aneuploidies.
So, the 10 Week Scan and NIPT are best seen as complementary tests: NIPT assesses selected genetic risks, while the scan assesses early fetal anatomy and markers of fetal health.
If something abnormal is suspected at the 10 Week Scan, we will explain the finding clearly, discuss what it may mean, and usually recommend a planned follow-up rather than making conclusions from one early scan alone. Depending on the finding, this may include extended NIPT, diagnostic testing such as CVS, or a targeted scan at 12–13 weeks to reassess the anatomy, NT and early heart development. In some cases, further specialist scans may also be arranged later in pregnancy, including a detailed anomaly scan and fetal heart scan. The aim is to give you earlier information, reduce uncertainty where possible, and create a clear, individual plan for the next steps.
A targeted follow-up scan at 12–13 weeks is often recommended because some structures become clearer as the baby grows, and some findings seen at 10 weeks need to be confirmed or reassessed. This scan allows us to review the NT, check whether any early concern has resolved, progressed or become more specific, and examine the anatomy in more detail, including the brain, spine, abdominal wall, limbs and early heart development. It is especially important when NT was increased, the 10 Week Scan was technically limited, or any structural concern was suspected. The aim is not simply to repeat the scan, but to use the extra development between 10 and 12–13 weeks to make the assessment more precise and guide the next steps.
A reliable 10 Week Scan should be performed by a specialist who is experienced in early fetal anatomy, high-resolution transvaginal ultrasound and first-trimester diagnosis. The fetus is very small at 10 weeks, so the scan requires excellent image optimisation, careful use of magnification, understanding of normal 10-week anatomy, and awareness of which structures can and cannot be assessed at this stage.
Experience with NT measurement at 10 weeks is particularly important, because the technique and interpretation are not the same as in the standard 11–13-week window. The sonographer also needs to recognise early signs of major structural problems, know when a finding is likely to be normal developmental variation, and understand when targeted follow-up or genetic testing should be recommended.
In addition, good practice should include ongoing audit, image review, peer feedback and correlation with 12–13-week and later pregnancy outcomes. In our view, the 10 Week Scan should not be treated as a routine “quick look” scan, but as a specialist early fetal assessment requiring appropriate training, equipment and quality assurance.
NT scan and NIPT at 10 weeks, then full results by week 12
1
If increased NT is found, you can have the SMART Test straight away
2
Receive genetic results in 2 weeks
3
Top-to-toe expert fetal examination
Disclaimer! These reflections are my own and arise from practice rather than committee. They do not represent the positions of the FMF, UCLH, NHS, RCOG, ISUOG, or any other organisation. As with any clinician, I may make mistakes or misjudgements. In my view, a carefully performed 10 Week Scan, used alongside appropriately selected modern NIPT and followed by targeted diagnostic testing when indicated, can provide a balanced clinical approach by supporting earlier risk assessment while avoiding unnecessary intervention or over-interpretation. Dr Fred Ushakov
For medical professionals who want to learn more about the SMART NT approach, access training, and join our clinical network.





