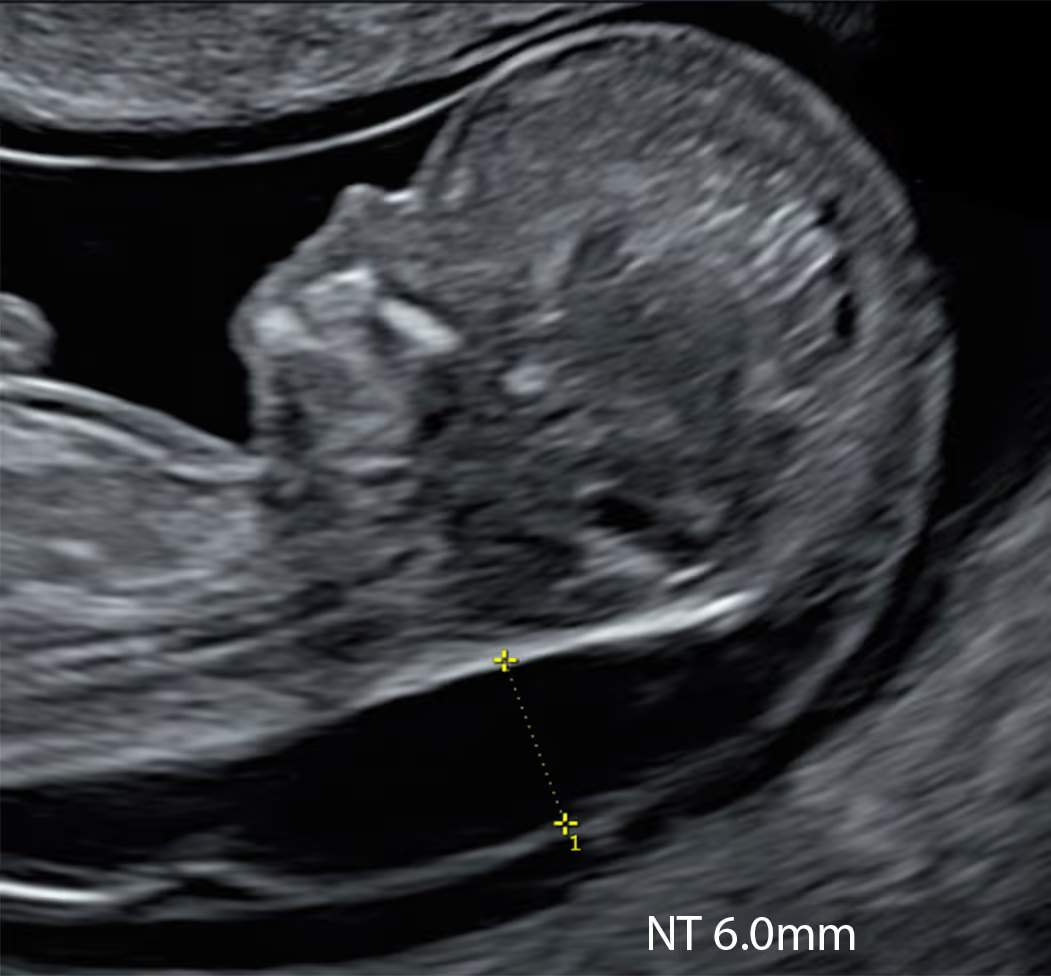
Has your baby been diagnosed with increased NT, early hydrops, or a cystic hygroma?
Act now to get answers and expert care.

While invasive diagnostic testing with CVS or amniocentesis remains the gold standard in pregnancies with increased NT, these tests have important limitations. They do not assess fetal structure and may not detect many monogenic disorders.
State-of-the-art non-invasive investigations can provide additional clinically relevant information without procedure-related risk.
TruCheck™ Early Cancer Screening is a blood test that can detect early signs of multiple cancers before symptoms appear

Has your baby been found to have an increased NT or hydrops before 11–14 weeks? Book SMART NT now.

Book an Early Fetal Echocardiography and consider the advanced KNOVA NIPT panel.

CVS does not test for most genetic disorders. Learn how to arrange whole genome sequencing (WGS) from your CVS sample.

This page is designed for UK-based patients. If you are worried about increased NT in your baby and would like more information or reassurance, you may wish to use the services of our partner clinics, London Pregnancy Clinic (LPC). LPC is a leading private UK facility specialising in targeted early fetal scanning, advanced NIPT, and extended genetic testing.
Unfortunately, we are not currently able to support families outside the UK.
If you would prefer the reassurance of NIPT from 10 weeks, rather than waiting until 12–13 weeks for Combined Test and NT assessment through the NHS, London Pregnancy Clinic (LPC) offers a unique early pregnancy pathway. LPC is currently the only clinic providing advanced 10-week fetal assessment before NIPT, using a structured scanning protocol that includes NT measurement.
If the scan is reassuring and the NT is below 2.5 mm, you can choose from a range of high-quality NIPT options. If the NT is increased (2.5 mm or more), the clinic can offer the SMART NT protocol, including KNOVA NIPT and a detailed follow-up scan at 12–13 weeks. The scan also include early fetal echocardiography to assess the baby’s heart.
Fortunately, increased NT at 10 weeks is uncommon (2-3%). The good news is that if the NT is normal at 10 weeks, it is extremely unlikely to increase later, making an early normal scan highly reassuring ahead of the routine 12-week NHS scan.
Many patients in the UK have a viability or dating scan either privately or through an NHS Early Pregnancy Assessment Unit (EPAU). If you are around 10 weeks pregnant at the time of your scan, it may be worth asking the sonographer, or doctor whether there is any concern about your baby’s NT.
At present, there is no national UK protocol for NT measurement at 10 weeks. Your clinician will usually explain this, and in many cases parents are advised to wait until the routine 12-week scan. However, if the NT appears visibly increased at 10 weeks and you ask about it, the clinician may discuss this finding with you. In some cases, they may describe the baby as “hydropic” or say that there is a large amount of fluid around the baby. This is understandably very worrying for parents.
In general, if the NT measures more than 3.5 mm at 11–14 weeks, parents should be referred to a Fetal Medicine Unit (FMU). At 10 weeks, however, there is currently no standard referral pathway, and most patients are advised to wait until the 12-week NT assessment.
London Pregnancy Clinic (LPC), as a leading provider of early fetal care in London, offers a solution for this situation through the SMART NT protocol. If you contact the clinic, they can arrange an urgent scan to reassess the NT using their structured 10 Week Scan protocol. You may then be offered the extended KNOVA NIPT, which screens for common chromosomal conditions associated with increased NT, as well as certain genetic conditions linked to increased NT, including Noonan syndrome and other RASopathies.
You may also be offered a follow-up scan at 12–13 weeks to assess how the NT is changing over time. In around half of cases, the NT resolves spontaneously within 1–2 weeks, which is generally associated with a better outcome. For parents who prefer a simpler approach, basic NIPT remains an option. Others may prefer to wait for the NHS scan at around 12 weeks and consider CVS, which is a diagnostic test.
If your baby has been found to have increased NT at the 11–14 week scan, the NHS will usually refer you to a Fetal Medicine Unit (FMU) for further assessment. You will normally be offered a more detailed review of the scan findings and discussion of the available testing options. Depending on the local pathway, this may include basic NIPT or invasive diagnostic testing such as CVS or amniocentesis. Further ultrasound follow-up may also be recommended, including assessment of the baby’s heart later in pregnancy, as increased NT can sometimes be associated with structural as well as genetic conditions.
For many parents, CVS can feel like a difficult decision. Although it is considered a diagnostic test, it is invasive, and some parents prefer to avoid it because of the small risk of miscarriage. In this situation, London Pregnancy Clinic (LPC) can offer a more detailed non-invasive pathway.
This may include specialist review, advanced NIPT, and structured follow-up scans to provide more information about the baby without the risks associated with invasive testing. This approach can be especially helpful for parents who would like further assessment but do not feel ready to proceed with CVS.
Advanced NIPT can screen for the main chromosomal conditions and, depending on the panel selected, some additional genetic conditions associated with increased NT. Follow-up scans can also help assess whether the NT is resolving and whether there are any early structural concerns, including possible heart abnormalities.
Although non-invasive testing cannot replace CVS or amniocentesis as a definitive diagnostic test, it can provide valuable additional information and closer monitoring. For parents who wish to avoid invasive procedures, LPC offers an expert early assessment pathway with personalised support, helping families better understand their options and plan the next steps with greater confidence.
Yes, CVS is considered the gold standard when increased NT is identified, because it is a diagnostic test for chromosomal conditions, including microdeletions and microduplications. However, standard CVS testing in the UK does not usually assess the many other genetic conditions that can also be associated with increased NT.
More advanced tests, such as whole exome sequencing (WES) and the more comprehensive whole genome sequencing (WGS), can look for a much wider range of genetic disorders. These tests can often be performed on the same CVS sample, so no further invasive procedure is needed. However, they are expensive and are not routinely offered to most parents when increased NT is the only finding.
Within the NHS, access to this type of advanced testing is governed by strict eligibility criteria under the Genomic Medicine Service (R21). For example, persistent increased NT may only qualify when there are additional structural abnormalities, and the exact criteria can change over time. It is therefore important to check with your NHS team whether your baby may be eligible.
One of the challenges is timing. In many cases, additional structural anomalies may not become apparent until the 20-week anomaly scan, which can delay access to advanced genomic testing and, in turn, delay important information for decision-making.
London Pregnancy Clinic (LPC) can support you in this situation with access to private whole exome sequencing (WES), whole genome sequencing (WGS), or the advanced KNOVA monogenic NIPT panel.
Private WES or WGS: What many parents do not realise is that a previously collected CVS sample may sometimes be transferred for private advanced testing, arranged through a specialist genetic consultant. This does not create any additional risk for the baby, as no further invasive test is required. London Pregnancy Clinic (LPC) can support this pathway by arranging a consultation with a genetic consultant, who can advise on extended testing and, where appropriate, organise transfer of the CVS sample to a specialist genetic laboratory.
Although WES and WGS can provide valuable additional information, they are expensive and the process can take considerable time.
KNOVA NIPT: If you have already had CVS but would like broader reassurance, KNOVA may offer a practical next step. Unlike standard NIPT, KNOVA includes a monogenic panel designed to screen for selected single-gene disorders relevant to increased NT, including conditions within the RASopathy spectrum such as Noonan syndrome. Because it is a targeted screen rather than a whole-exome or whole-genome test, it is typically a more cost-conscious option and is designed to deliver results more quickly.
For many families, this makes KNOVA an attractive intermediate option after CVS: broader than routine CVS chromosomal testing, faster than WES or WGS, and without the cost or delay of more extensive genomic analysis. It is important, however, to understand its role clearly. KNOVA remains a screening test, not a diagnostic test, and because it uses a restricted monogenic panel, a normal result cannot exclude all genetic conditions associated with increased NT. Where deeper analysis is needed, WES or WGS may still be considered through a specialist genetics pathway.
Disclaimer! These reflections are my own and arise from practice rather than committee. They do not represent the positions of the FMF, UCLH, NHS, RCOG, ISUOG, or any other organisation. As with any clinician, I may make mistakes or misjudgements. But I believe that coupling a careful 10 Week Scan with modern NIPT, and escalating to targeted diagnostics when indicated, offers families the balance we seek: early clarity without haste, and precision without noise.
No. The NHS does not routinely perform formal NT measurements at 10 weeks. In the NHS screening programme, NT is measured as part of the combined test only when the baby’s crown–rump length is 45–84 mm, which corresponds to about 11 weeks and 2 days to 14 weeks and 1 day of pregnancy.
A blood sample for combined screening can be taken from 10 weeks, but the ultrasound NT measurement itself is not part of the standard NHS pathway at that stage. Some parents may have an earlier viability or dating scan around 10 weeks, and a clinician may notice increased fluid, but this is outside the routine NHS NT screening window.
No. In the UK, there is no specific national requirement to perform a formal NT assessment or automatic referral before the standard NHS combined screening window. Within the NHS screening programme, NT is used as part of the combined test only once the baby is large enough for a validated measurement, which is generally from 11 weeks plus 2 days onwards (CRL 45 mm and more). Before that point, there is no established national pathway for early increased NT, and NT should not be interpreted in the same formal way as it is at the routine 11–14 week scan.
In practice, this means that communication can be variable. If a sonographer or doctor sees a possible increase in fluid behind the baby’s neck before 11 weeks, they may decide not to present this as a formal abnormal NT finding, particularly when there is no NHS protocol, no clear referral route, and the standard plan would usually be repeat assessment at the routine 12-week scan. Some clinicians may feel that raising the issue too early could create significant anxiety for parents at a stage when the finding may still be uncertain and when formal screening criteria have not yet been met. This is better described as cautious or inconsistent early disclosure, rather than a defined rule not to tell parents.
That said, doctors still have a general professional duty to communicate relevant information honestly and to support informed decision-making. So while there may be no specific obligation to disclose “increased NT” before 11 weeks as a formal screening diagnosis, there is still an ethical expectation to be open if a potentially important concern is seen, especially if parents ask directly about the appearance of the scan. In those situations, clinicians may explain that the finding is not yet part of the validated NHS NT pathway, but that there appears to be increased fluid or a possible early concern that should be reassessed.
SMART NT is a specialised adaptation of the SMART Test® for pregnancies in which increased NT is identified at 10 weeks. The SMART NT protocol is designed specifically for the management of early increased NT and includes confirmation of increased NT (above 2.5 mm), KNOVA NIPT, and a detailed follow-up targeted scan at 12–13 weeks. SMART Test® is a registered trademark of London Pregnancy Clinic.
If your baby’s NT is normal at 10 weeks, this is very good news. You can still choose further testing for added peace of mind through the SMART Test®. SMART Test® combines an advanced 10-week scan with an extended NIPT panel, and London Pregnancy Clinic currently offers SMART Test® KNOVA and SMART Test® Plus as part of this pathway.
Unlike SMART NT, the standard SMART Test® does not routinely include an early follow-up fetal scan, although this can be arranged separately. In this situation, we would usually recommend an Early Fetal Scan slightly later, at around 14–16 weeks, when the baby’s anatomy is more developed and a wider range of structural abnormalities can be assessed.
KNOVA is an important part of the assessment, but it does not replace specialist ultrasound. While KNOVA can screen for selected chromosomal and monogenic conditions associated with increased NT, only expert scanning can assess the baby’s anatomy and look for major structural abnormalities, including early signs of congenital heart disease.
At London Pregnancy Clinic (LPC), both scans play a distinct and valuable role. The 10 Week Scan helps exclude major and potentially lethal structural abnormalities that may not be linked to a detectable genetic syndrome. The 12–13 week targeted scan (Early Fetal Scan and Early Echocardiography) provides a more detailed anatomical review, with particular attention to abnormalities associated with increased NT, especially cardiac defects.
Although these scans can be delayed and performed later within the NHS or elsewhere, early specialist assessment may identify an underlying structural cause much sooner. If increased NT is related to a structural problem, it is often more helpful to detect this on an expert targeted scan at the earliest possible stage, rather than waiting for it to declare itself later in pregnancy.
A 10-week specialist scan does not replace the routine NHS 12-week scan, but it can provide important information earlier. In the NHS, formal NT measurement is part of the combined screening pathway only when the baby’s crown–rump length is 45–84 mm, which corresponds to about 11 weeks and 2 days to 14 weeks and 1 day. By contrast, the national NHS pathway for structural anomaly screening is the 20-week anomaly scan, performed between 18+0 and 20+6 weeks, when the baby is screened for 11 physical conditions.
This means the routine NHS 12-week scan does check NT, but it is not the national screening pathway for detailed structural assessment of the fetus. Some NHS units do look carefully at early fetal anatomy at 12 weeks, and obvious severe abnormalities may sometimes be suspected at that stage, but this is not the same as a nationally standardised first-trimester anomaly screening programme.
For that reason, an earlier specialist scan at 10 weeks may be helpful if you want information sooner rather than waiting for the routine NHS pathway. It can allow earlier specialist review, earlier planning, and in some cases earlier recognition of major concerns that might otherwise only become clear later in pregnancy. It is also reasonable to ask your NHS provider exactly what they assess structurally at the 12-week scan, particularly whether they actively look for major abnormalities such as severe heart defects or open spina bifida, as these are among the types of physical conditions formally screened for later in the NHS anomaly pathway.
The short answer is that, under current NHS practice, most severe fetal anomalies (67.3%) are not detected in early pregnancy.
YYou can find the extended analysis of the situation in the UK in this very recent study published in November 2025: Karim et al., Impact of First-Trimester Ultrasound on Early Detection of Major Fetal Anomalies: Nationwide Population-Based Study of Over 1 Million Pregnancies.
This nationwide study should serve as a wake-up call for UK prenatal care. In a population-based analysis of more than 1 million pregnancies across England, only 32.7% of 14 major fetal anomalies were identified before 16 weeks. In other words, around two-thirds had still not been diagnosed by that stage, meaning that for most affected families, important information was delayed until mid-pregnancy or even later.
The study is especially important because 12 of these 14 anomalies are already included in the NHS Fetal Anomaly Screening Programme for the second trimester, at the 20-week scan. This means the problem is not that these conditions are too rare or too obscure to matter; they are major anomalies that the NHS already recognises as important targets for screening. Yet in practice, early detection remains limited and highly variable.
Some of the findings are genuinely alarming. Acrania, one of the commonest, most severe, and most readily recognisable lethal anomalies, was still not identified before 16 weeks in more than 5% of affected pregnancies. For a condition of this severity, any delay in diagnosis matters.
This study is also powerful because it is the first to describe first-trimester anomaly screening practice at population level in England. It included 110 NHS trusts, had an 84% response rate, covered more than 1 million pregnancies, and included every region of the country. These are not isolated observations from a few specialist centres. They are real-world national data showing that the absence of standardised first-trimester structural screening leads to variation, inequity, and delayed diagnosis.
The earliest scan that can give some reassurance about your baby’s heart is a specialist early fetal heart scan, also called an early fetal echocardiogram, at around 12 weeks. In experienced fetal cardiology centres, this scan can detect many major or severe heart defects. Studies in high-risk pregnancies suggest that around 80% of major cardiac abnormalities may be identified at this stage.
However, the baby’s heart is still very small at 12 weeks, so a transabdominal scan may not always provide all the answers. At 11–14 weeks, a transvaginal approach can improve image resolution and may add important detail, especially when combined with the usual transabdominal scan. For this reason, if you are arranging an early fetal heart assessment, it is sensible to ask whether the centre or specialist is experienced in transvaginal early fetal echocardiography before booking.
Transvaginal early fetal echocardiography can be performed in experienced hands up to about 16 weeks, but it still does not replace the standard detailed fetal heart scan later in pregnancy, usually at around 18–22 weeks. A normal scan at 12 weeks cannot exclude all heart problems, particularly more moderate or minor defects, and some abnormalities only become apparent as the heart develops further. Increased nuchal translucency is one of the recognised reasons for offering this extra cardiac assessment.
Because CVS answers only one part of the question. It is excellent for diagnosing or excluding the main chromosomal abnormalities, but it does not assess the baby’s anatomy, it does not diagnose congenital heart defects, and it does not rule out many single-gene conditions that can also present with increased NT. Increased NT is linked not only to chromosomal problems, but also to major structural abnormalities and a wide range of genetic syndromes, even when the CVS result is normal.
This is why additional assessment is often recommended after a normal CVS result. Detailed follow-up ultrasound helps look for structural anomalies that may only become visible later, and fetal echocardiography may be advised because increased NT is associated with a higher risk of congenital heart disease even in chromosomally normal babies.
A further reason is monogenic syndromes. Some conditions, particularly Noonan syndrome and other RASopathies, can be associated with raised NT but will not usually be detected by standard CVS chromosome testing. In selected cases, this is why clinicians may discuss additional genomic testing such as targeted monogenic panels, exome sequencing, or genome sequencing.
R21 is the NHS rapid prenatal exome sequencing pathway in the National Genomic Test Directory. In simple terms, it is a fast genomic test used in ongoing pregnancies when doctors think there may be an underlying single-gene condition and a molecular diagnosis could change pregnancy management. It uses invasive prenatal sampling and is usually requested by a clinical geneticist after multidisciplinary discussion with fetal medicine.
In the setting of increased NT, R21 is not usually the first test for an isolated raised NT. For an isolated NT over 3.5 mm, the usual starting point is chromosomal testing. R21 comes into the picture when the findings suggest a higher chance of a monogenic disorder, particularly if the NT is over 6.5 mm between 11 and 14 weeks and there is at least one additional anomaly, or if there is persistent NT over 3.5 mm together with structural abnormalities in two or more systems. It may also be used in parallel with chromosome testing when increased NT is seen alongside multiple congenital anomalies that would qualify for R21 anyway.
So, in practical terms, R21 is the NHS route to rapid fetal exome testing when increased NT is part of a more complex picture, rather than a stand-alone test for every baby with raised NT. The exact eligibility is determined by the fetal medicine and genetics team, and the criteria can be updated over time.
If you are aware that a standard NHS CVS sample is usually tested only for chromosomal conditions and copy number changes such as microdeletions and microduplications, it is important to understand what this does not exclude. Many genetic syndromes linked with increased NT, including conditions such as Noonan syndrome and Kabuki syndrome, are caused by single-gene changes and would not usually be diagnosed by standard NHS chromosome testing alone. In this situation, some parents wish to consider whole exome sequencing (WES), or in some cases the more comprehensive whole genome sequencing (WGS).
The first step is to ask your NHS Fetal Medicine Unit whether further testing may be possible through the NHS via the R21 rapid prenatal exome sequencing pathway. If the answer is yes, this may allow you to have the test without private cost. NHS rapid prenatal exome results are typically reported in around 3 to 4 weeks, although timings can vary. If your NHS team do not feel that R21 is available in your case, the situation becomes more complicated. The CVS sample is usually held in a regional genetics laboratory or Genomic Laboratory Hub, and if you wish to pursue private testing, arrangements may need to be made for the sample to be released and transferred to a specialist laboratory. This process can be logistically difficult, may involve secure medical courier transfer, and can be expensive.
This is why it is often best to work with a private provider specialising in both fetal ultrasound and genomics, who can coordinate the pathway properly. A very important first step is a private targeted specialist scan, because this may identify structural findings associated with increased NT. If additional abnormalities are found, you may then become eligible for NHS R21 testing and may not need expensive private exome sequencing. If the baby appears structurally normal, the next step is usually detailed counselling with a consultant clinical geneticist, who can explain whether WES or WGS is more appropriate in your situation and help guide the process of sample transfer and further testing. Some private clinics have expertise with this pathway, including London Pregnancy Clinic (LPC), where the process may include a targeted scan, specialist counselling, and support with the practical steps needed if private genomic testing is chosen.
For medical professionals who want to learn more about the SMART NT approach, access training, and join our clinical network.

Lorem ipsum dolor sit amet conse ctetur adip iscing elit justo quis odio sit sit ac port titor sit males dolor sit consectur dolor.

Lorem ipsum dolor sit amet conse ctetur adip iscing elit justo quis odio sit sit ac port titor sit males dolor sit consectur dolor.

Lorem ipsum dolor sit amet conse ctetur adip iscing elit justo quis odio sit sit ac port titor sit males dolor sit consectur dolor.

Lorem ipsum dolor sit amet conse ctetur adip iscing elit justo quis odio sit sit ac port titor sit males dolor sit consectur dolor.

Lorem ipsum dolor sit amet conse ctetur adip iscing elit justo quis odio sit sit ac port titor sit males dolor sit consectur dolor.

Lorem ipsum dolor sit amet conse ctetur adip iscing elit justo quis odio sit sit ac port titor sit males dolor sit consectur dolor.





