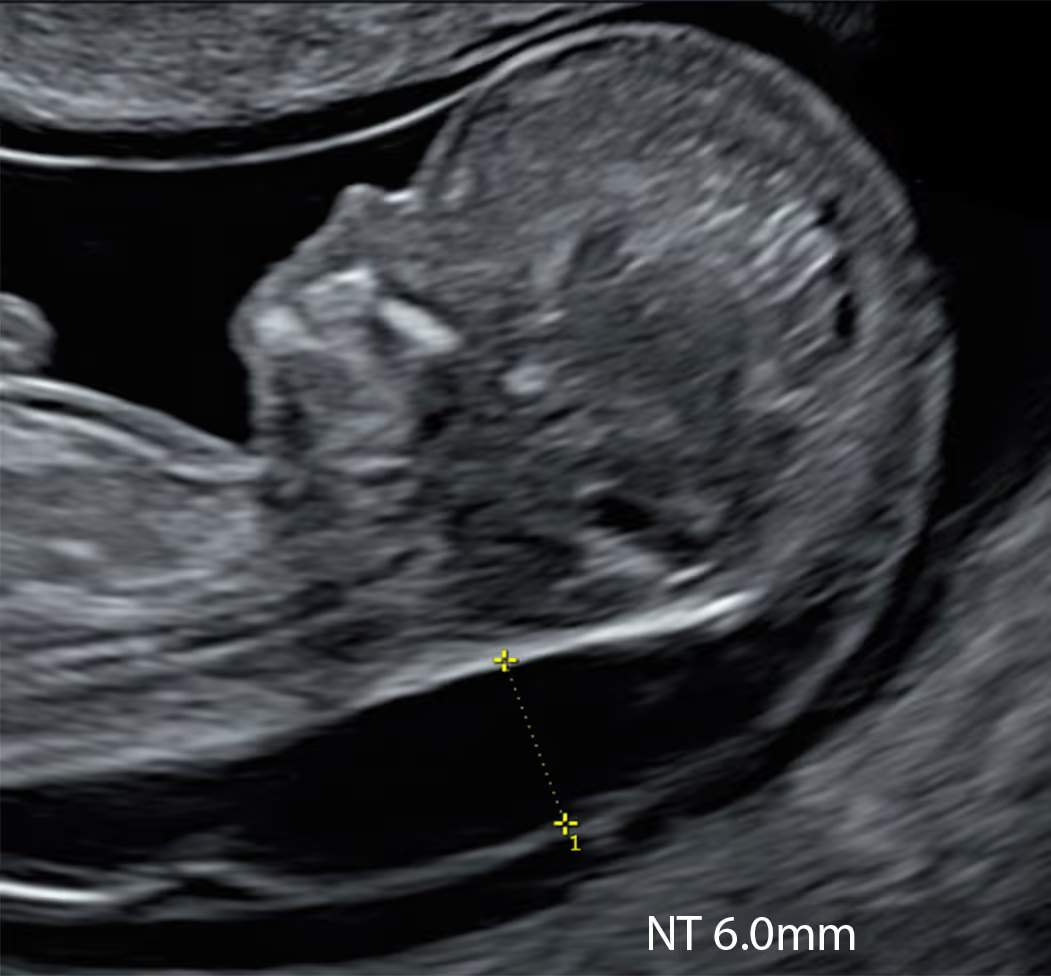
SMART NT scans focus on detecting early structural anomalies, not just measuring neck fluid.

The 10 Week Scan is the principal screening scan for NT measurement and can also identify some lethal anomalies. If increased NT is detected, it triggers the SMART NT protocol.
A targeted follow-up scan for fetuses with increased NT. It assesses structural anomalies associated with high NT and evaluates the progression of NT - whether it has resolved or remains persistent.
The two-step scan protocol offers clear advantages over current methods. It allows the earliest detection of increased NT, identifies related structural anomalies (especially heart defects), and monitors how the NT changes over time. These changes - resolution, persistence, increase, or progression to early hydrops or cystic hygroma - are prognostically important for the baby’s outcome.

Learn More about the SMART Protocol
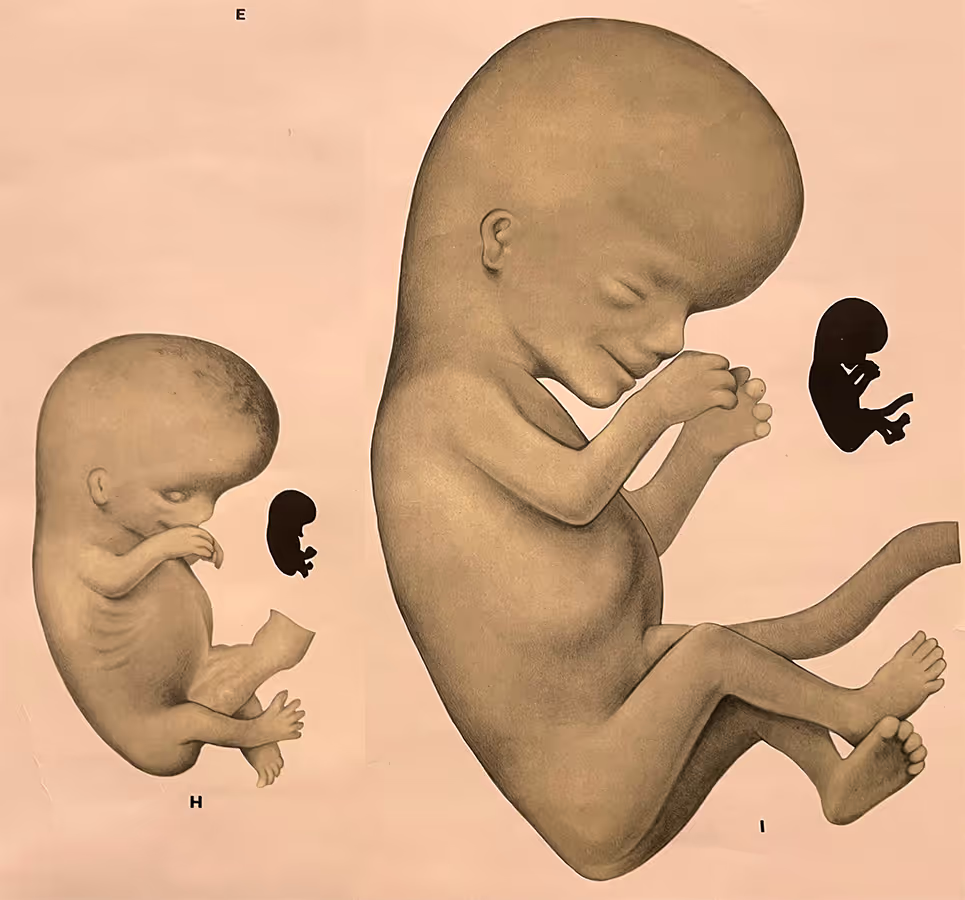
During this two-week period (10 to 12 weeks), the fetus undergoes rapid growth and maturation. The crown–rump length (CRL) doubles from about 3 cm to 6 cm, and major developmental changes occur in the brain, skeleton, abdominal wall, kidneys and other organs. From a scanning perspective, extensive evidence and international guidelines confirm that by 12–13 weeks, the fetal anatomy can be comprehensively assessed from head to toe using a protocol comparable to the standard 20-week anomaly scan. Results of genomic NIPT are also typically available within about two weeks.

Learn More about the SMART Protocol
The initial and follow-up scans serve very different purposes. The 10 Week Scan is a screening examination that should be performed for every woman to identify high-risk fetuses with increased NT. The 12–13 Week Scan is a targeted diagnostic assessment performed by a fetal medicine specialist with expertise in early anomaly detection, particularly fetal cardiac evaluation. Together, these two scans provide both early risk identification and specialist confirmation, helping to ensure that no structural problems are missed.
Learn More about the SMART Protocol
Babies with increased NT are at higher risk of serious heart defects. Multiple studies show that 50–80% of major cardiac anomalies can be detected at 12–13 weeks. In our experience, when increased NT or early hydrops is caused by a heart defect, it is usually identifiable by an expert first-trimester echocardiographic scan.
vAn Effective Two-Step Screening Protocol with Three Key Elements
1
If increased NT is found, you can have the SMART Test straight away
2
Receive genetic results in 2 weeks
3
Top-to-toe expert fetal examination
Disclaimer! These reflections are my own and arise from practice rather than committee. They do not represent the positions of the FMF, UCLH, NHS, RCOG, ISUOG, or any other organisation. As with any clinician, I may make mistakes or misjudgements. In my view, a carefully performed 10 Week Scan, used alongside appropriately selected modern NIPT and followed by targeted diagnostic testing when indicated, can provide a balanced clinical approach by supporting earlier risk assessment while avoiding unnecessary intervention or over-interpretation. Dr Fred Ushakov
Conditions associated with high Nuchal Transluncency (NT)





Increased NT Cut-off day by day chart.
Because earlier information changes what you can do, and when.
- Earlier reassurance: many parents want a reliable early check as soon as it’s feasible.
- Earlier risk identification: if the NT is clearly increased at 10 weeks, it can be an early marker for chromosomal, genetic or structural problems.
- Earlier genetics pathway: doing the scan at 10 weeks allows NIPT to be started promptly, so results are usually available by around 12 weeks, rather than later.
- A planned second look: SMART NT is a two-step approach—the follow-up targeted scan at 12–13 weeks checks detailed early anatomy, the heart, and how the NT is evolving (NT dynamics), which helps refine risk and next steps.
- More time for decisions and support: if something is concerning, families have more time for counselling, referrals, and (if needed) diagnostic testing.
SMART NT doesn’t replace the standard mid-pregnancy anatomy scan; it’s designed to bring meaningful screening forward and then confirm and expand the assessment at 12–13 weeks.
No. We’re not suggesting two scans for everyone. Instead, we have developed a new model of earliest first-trimester screening that is earlier and better than the current Combined Screening Test (CST) model.
We’re proposing to replace the outdated CST (12-week NT + blood tests) with a single, earlier “one-stop” visit: a 10-Week Scan plus NIPT (a detailed earliest anatomical scan and a genomic test based on fetal cfDNA). At 10 weeks we also measure the NT, and if it is increased (2.5 mm or more) we offer the SMART NT protocol, which includes an expert targeted scan at 12–13 weeks. Only a small proportion of the population with early increased NT (around 2–3%) will need this additional targeted scan.
There are a few other situations where a second scan may be needed even when the NT is normal - for example, if the 10-week anatomy/NT assessment is technically limited, or if we need a focused re-check because of a suspected structural concern (for example, a possible heart defect or spina bifida).
Definitely not - we generally still recommend attending the routine NHS 11–14-week scan (or government funded scans in other countries), even if your 10-week scan and NIPT are normal.
Our approach can replace the Combined Screening Test (NT + bloods) as a screening strategy in the future, but it doesn’t fully replace the NHS visit because the NHS scan also provides: official dating/EDD and documentation for your NHS pregnancy record, an additional structured assessment at 12–13 weeks for some abdominal wall defects, facial anomalies and kidneys/bladder conditions, and in some hospitals, pre-eclampsia (PET) screening (often using a combined risk assessment with blood pressure and blood tests/Dopplers).
Some people do choose to opt out, but it’s best done in discussion with your NHS team so your care pathway and any additional screening (such as pre-eclampsia screening) isn’t missed.
If the 10 Week Scan is normal (no major structural concerns and the NT is normal) and the NIPT result is low chance, we would usually recommend the next specialist scan as an early fetal scan (early anomaly scan) between 14 and 16 weeks.
As mentioned in the Q&A above, we still recommend attending the routine NHS 11–14-week scan (which is traditionally part of the Combined Screening Test pathway) because it is an important part of NHS maternity care, documentation, and in some hospitals may also be combined with additional screening such as pre-eclampsia risk assessment. However, from the perspective of the best timing for early structural assessment, 14–16 weeks is often the most informative next step.
In our experience, the 11–14-week scan typically adds only a limited amount of new anatomical information after a high-quality 10-week examination, as it is largely looking for the same severe anomalies. It is very uncommon for a significant structural finding to be completely absent at 10 weeks yet clearly present at 12–13 weeks. At the same time, there are important conditions that may develop or become obvious shortly after a “normal 12-week scan”, such as congenital diaphragmatic hernia (CDH), congenital high airway obstruction syndrome (CHAOS), lower urinary tract obstruction (LUTO), evolving skeletal dysplasias, some forms of hypoplastic left heart syndrome (HLHS), as well as other serious abnormalities. Leaving the next detailed assessment too late (around 20 weeks) can reduce the chance of picking these up early.
The 14–16-week visit can also be used to assess cervical length in higher-risk situations, and many women find a scan around 16 weeks particularly reassuring because it confirms that the pregnancy is progressing well.
We generally do not recommend routine scans in the 16–18-week window because the fetal position at that stage is often awkward (commonly a “sitting” posture), which can make the examination technically more challenging and less consistently diagnostic.
It is a different type of appointment, with a different purpose, and it is performed by an expert in early fetal anatomy rather than a screening-only clinician.
A standard 11–14-week NT scan is a screening scan designed to measure the nuchal translucency and, in many settings, combine this with blood markers and maternal age to estimate the chance of the common trisomies (T21, T18 and T13).
The SMART NT 12–13-week scan is a planned, targeted assessment for pregnancies where an increased NT was already identified around 10 weeks. By this stage, major early anomalies have usually been excluded and, in most cases, results from an extended NIPT (such as KNOVA by Fulgent) are already available. The focus is a detailed early anatomy review, with particular attention to structures linked with increased NT, especially the heart, using a structured protocol that mirrors, as far as possible at this gestation, the approach of a standard 20-week anomaly scan.
In most cases, no - we do not ask patients to have a full bladder for either scan. A full bladder can be uncomfortable and it often doesn’t improve image quality at these gestations, or even reduce resolution. In early pregnancy, an overly full bladder can push the uterus into a less favourable position and may make the scan more difficult. With modern high-resolution ultrasound, we usually obtain excellent views with a comfortably empty (or only mildly filled) bladder. If we need more detail we will offer a transvaginal scan (TVS), which require an empty bladder. Occasionally, if the uterus is positioned deep in the pelvis or views are limited by large fibroids, we may suggest drinking a small amount of water, but this is the exception rather than the rule.
Historically, transabdominal pelvic ultrasound used a full bladder as an acoustic window to improve views, a technique developed by ultrasound pioneer Prof Ian Donald (Glasgow, UK) in the early 1960s. Modern high-resolution ultrasound (with high-frequency probes and advanced image processing) provides far better diagnostic detail, so a full bladder is usually unnecessary, especially when transvaginal scanning is available.
For medical professionals who want to learn more about the SMART NT approach, access training, and join our clinical network.





